냉동지방분해술 이후에 발생한 노신경병증 증례
Radial Neuropathy after Cryolipolysis
Article information
Trans Abstract
Cryolipolysis has become available for the noninvasive reduction of adipose tissue. A 33-year-old woman presented with wrist drop of the right arm that had first appeared 7 days previously. She had undergone cryolipolysis on both upper arms immediately prior to the onset of symptoms. A nerve conduction study showed radial neuropathy proximal to the elbow, and ultrasonography revealed focal swelling of the radial nerve at the spiral groove. Although cryolipolysis has been known as a safe method, nerve injury can result from compression and/or hypothermia during the procedure.
냉동지방분해술(cryolipolysis)은 피하지방의 온도를 낮추어 지방분해를 유도하는 기술이다[1]. 냉동지방분해술은 미국 식품의약국(food and drug administration, FDA)의 승인을 받은 시술로 종아리, 옆구리, 배 등 선택적으로 적용이 가능하고 비침습적이어서 상업적으로 널리 이용되고 있다. 비침습적이면서 주위 정상조직의 손상을 유발하지 않는 것이 장점이며, 일시적인 멍(bruise), 감각장애, 통증 등 경미한 부작용이 보고되었다[2-4].
저자는 냉동지방분해술 이후에 발생한 노신경병증 환자를 경험하여 증례보고와 함께 신경손상 기전에 대해 고찰하였다.
증 례
33세 여자환자로 1주일 전에 발생한 오른손의 근력약화로 내원하였다. 환자는 일주일 전에 한의원에서 냉동지방분해술을 1차례 받았고, 시술이 끝나자 마자 오른손의 근력약화를 인지하였다. 냉동지방분해술은 냉동지방분해장치(Cool Sculpting®; Zeltiq Aesthetics, Pleasanton, CA, USA)를 이용하여 엎드린 자세에서 양측 위팔의 뒤가쪽에 30분간 시행했다. 과거력에서 특이 병력은 없었고 가족력 및 약물 복용력에서 특이사항은 없었다. 신경학적 진찰에서 의식은 명료하였고 뇌신경기능은 정상이었다. 근력은 오른쪽 손목과 손가락을 펼 때 Medical Research Council (MRC)등급 II였고, 다른 부위의 근력은 정상이었다. 감각검사에서 오른쪽 손등의 감각저하와 이상감각이 보였다. 심부건 반사는 팔다리에서 모두 감소되었으나 대칭적이었고, 바빈스키 징후는 보이지 않았다.
증상 발생 10일 후에 시행한 신경전도검사에서 오른쪽 노신경에서 복합근육활동전위 진폭의 감소를 보였고, 팔꿈치와 겨드랑이 사이에서 전도차단이 보였다. 얕은노신경의 감각신경전도 검사는 정상이었다(Table). 정중신경과 자신경의 신경전도검사는 모두 정상이었다.
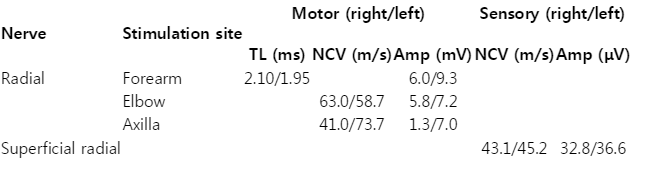
Nerve conduction study findings
신경근육초음파(Fig.)에서 노신경고랑(radial spiral groove)에서 오른쪽 노신경의 단면적이 8.8 mm2 로 커지고 에코음영이 감소하였다(Fig. B). 같은 위치에서 검사한 왼쪽 노신경의 단면적은 4.0 mm2 로(Fig. E) 오른쪽이 왼쪽의 2배 이상이었다. 노신경고랑 위아래에서는 다시 정상크기를 보였다(Fig. A, C). 임상증상과 검사결과를 토대로 노신경고랑에서 발생한 노신경병증으로 진단하고 고용량(하루 50 mg) 스테로이드를 1주일간 경구 투약하였다. 환자의 증상은 서서히 회복되어 4주 후에는 MRC Ⅳ로 근력이 회복되었다.
Ultrasound images show the radial nerve at the level of spiral groove. (A-C) Transverse view of the right radial nerve (arrowhead). (B) The CSA of the nerve at the level of spiral groove is increased at 8.2 mm2. (A, C) The CSA of the nerve distal and proximal to the swelling is approximately 4.2 and 5.2 mm2 , respectively. (D-F) The left radial nerve in the similar location is of normal echogenicity and size (4-4.2 mm2 ). (G) In the photo of patient, the white dotted line indicates the attachment site of cooling plate. BR; brachioradialis, h; humerus, Br; brachialis, CSA; cross-sectional area.
고 찰
노신경마비는 노신경고랑부위에서 신경이 압박되거나 외상에 의해 주로 발생한다. 해부학적으로 노신경이 위팔뼈의 노신경고랑 부위를 돌아서 내려오기 때문에 이 근처에서 외부의 압박에 특히 취약하다. 증례에서 신경전도검사는 병변의 대략적인 위치가 전도 차단이 있는 겨드랑과 팔꿈치 사이임을 알려주고, 초음파검사는 정확한 병변위치가 노신경고랑임을 보여준다. 병변부위에서 신경의 단면적이 증가하고 에코음영이 감소하는 것은 압박신경병증의 대표적인 초음파 소견이다[5]. 증상 발생 후 10일째 시행한 신경전도 검사에서 노신경에서 전도차단이 보이고 얕은노신경에서 정상소견이 보이는 것으로 볼 때 주된 병태생리는 축삭보다는 수초의 손상으로 판단된다[6].
미용목적으로 지방을 제거하는 대표적인 시술인 지방흡인술(liposuction)은 폐색전증과 같은 심각한 합병증이 있어 비침습적인 시술에 대한 요구가 지속적으로 있었다. 피하지방이 저온에 노출되면 지방조직이 손상을 받으면서 소엽지방층염(lobular panniculitis)이 유발된다[1]. 소엽지방층염으로 인해 염증 매개 물질과 사이토카인이 방출된다. 염증 세포는 지방조직을 포식하여 지방을 제거하고, 지방감소는 저온 노출 후 평균 3개월에 걸쳐서 지속된다. 멍이나 통증과 함께 감각이상이 발생하는 경우가 있지만 시술 후 시행한 피부 생검을 통해 표피 밑 신경 얼기의 구조적인 변화가 없는 것이 확인되었고, 감각이상도 일시적인 것으로 보고되었다[7]. 부작용으로 말초신경병증이 발생한 보고는 현재까지 한편이 확인되었고, 본 증례처럼 위팔에 시술 후에 노신경마비로 생각되는 신경병증이 발생하였다[8]. 하지만, 이 보고는 신경병증의 병변위치나 병태생리 및 기전보다는 말초신경병증의 발생자체를 중점적으로 기술하였다.
일반적인 시술과정은 지방을 제거할 부위에 사각형의 냉각판을 대고 음압을 가해 지방을 포함한 조직을 당긴 뒤 섭씨 10도 정도로 냉각하여 30분에서 1시간 정도 유지한다[4]. 증례에서 병변부위가 노신경의 흔한 압박부위인 노신경고랑이므로 주된 원인은 음압을 가하면서 냉각판이 너무 강하게 고정되어 냉각판과 위팔뼈 사이에서 신경이 압박된 것으로 판단된다. 하지만 저체온도 말초신경병증을 유발할 수 있고[9] 압박신경병증의 발생위험을 증가시키는 요인이다[10]. 30분이라는 비교적 짧은 시간 동안 압박된 후에 발생한 점을 고려할 때, 냉각에 의한 국소적 저체온으로 인해 노신경이 압박 손상에 취약한 상태가 되었다고 볼 수 있다. 또한 냉각에 의해 감각이 무뎌져서 환자가 의식이 명료한 상태임에도 불구하고 신경 손상에 의한 통증과 이상감각을 시술이 끝날 때까지 인지하지 못한 것도 하나의 요인이다.
냉동지방분해술은 안전성을 장점으로 널리 사용되는 시술이지만, 냉각판을 밀착시키는 과정에서 압박신경병증이 발생할 수 있다.