척추동맥기시부협착 진단을 위한 경동맥초음파촬영술과 컴퓨터단층혈관조영술 또는 자기공명혈관조영술 비교
Carotid Ultrasonography vs. CT or MR Angiography in the Diagnosis of the Stenosis of Vertebral Artery Origins
Article information
Trans Abstract
Background:
The origin of the vertebral artery (VA) is prone to be misinterpreted as having focal stenosis on computed tomography angiography (CTA) or magnetic resonance angiography (MRA) due to artifacts. Ultrasonography may be a valuable technique to reveal stenosis of the VA origin. We compared the findings for the VA origin from CTA or MRA with those from ultrasonotraphy.
Methods:
We consecutively enrolled patients who underwent angiography (CTA or MRA) and carotid ultrasonography. The V2 and V1 portions of the VA were insonated to evaluate the presence of plaque or steno-occlusion. CTA or MRA data were evaluated. Stenosis or occlusion of the VA origin was categorized as present or absent. The results from the two methods were compared.
Results:
The mean age of the 73 investigated patients was 61.1 years, and 46 (63.0%) of them were male. Among the 22 patients with steno-occlusion of the right VA on CTA or MRA, only six had stenosis on ultrasonography. Regarding the left VA, only four patients among 16 who showed steno-occlusion on CTA or MRA had steno-occlusion on ultrasonography. The level of agreement between the two methods was 82.2% on the left side and 75.3% on the right side. There were no clinical differences between the patients with and without false-positive results on CTA or MRA.
Conclusions:
In 16.4% (left) and 21.9% (right) of all patients, lumens with steno-occlusions observed on CTA or MRA were revealed as normal on ultrasonography. The diagnosis of VA origins could be improved by applying these two methods complementarily.
서 론
후순환뇌경색은 전체 허혈뇌경색의 4분의 1을 차지한다. 그 중 척추동맥으로부터의 동맥-동맥색전증이 후순환뇌경색 원인의 4분의 1이 된다고 한다[1]. 명백한 혈관협착과 심장질환이 없는 후순환뇌경색은 컴퓨터단층혈관조영술에서 관찰하지 못한 척추동맥기시부의 동맥경화에 의하여 발생할 수도 있다. 따라서 척추동맥기시부협착을 정확하게 진단한다면 보다 적절한 뇌졸중의 예방치료를 할 수 있을 것이다.
척추동맥의 V1분절의 기시부는 동맥경화에 취약한 부분이다[2]. 그러나, 컴퓨터단층혈관조영술이나 자기공명혈관조영술에서 관찰되는 척추동맥기시부는 흐름허상(flow artifact) 때문에 마치 협착이 있는 것처럼 오인될 수 있다. 이러한 상황에서, 두개외척추동맥의 초음파촬영술은 척추동맥협착의 직접적 또는 간접적인 근거를 제공하는 검사법이 될 수 있다. 따라서, 컴퓨터단층혈관조영술 및 자기공명혈관조영술에서 관찰되는 척추동맥기시부 소견을 경동맥초음파촬영술을 통한 검사결과와 비교하여 두 검사법의 차이와 초음파촬영술의 필요성을 알아보고자 한다.
대상과 방법
본원 신경과에서 경동맥초음파촬영술과 뇌혈관조영술(컴퓨터단층혈관조영술 또는 자기공명혈관조영술)을 모두 시행한 환자를 연속적으로 등록하였다. 나이, 성별, 고혈압, 고지혈증, 당뇨병, 흡연력을 조사하였고, 뇌혈관조영술에서 관찰된 혈관협착 여부를 임상변수로 수집하였다. LOGIQ 7.0 (General Electronics, Milwaukee, WI, USA)을 사용하여 한 명의 검사자가 경동맥초음파촬영술을 하였다. 척추동맥의 V1, V2분절을 B모드영상을 통하여 플라크 또는 협착과 폐색을 관찰하였다. 저에코플라크에 의한 협착을 진단하기 위하여 칼라도플러검사의 혈류속도를 참고하였다. 척추동맥기시부를 검사하기 위하여 탐색자의 머리쪽 끝 또는 발쪽 끝을 기울여 탐색자 표면과 혈관 사이의 각을 적당히 만드는 힐앤토기법(Heel and toe technique)을 사용하였다[3]. 컴퓨터단층혈관조영술 또는 자기공명혈관조영술에서의 척추동맥기시부협착 소견은 임상변수를 모르는 연구자가 독립적으로 평가하였다. 척추동맥형성저하증으로 판단한 경우, 즉 혈관직경이 3 mm 미만이며, 고저항혈류양상을 보이는 경우는 연구대상에서 제외하였다. 컴퓨터단층혈관조영술은 LightSpeed VCT (General Electric Medical System, USA)로 촬영되었다. 삼차원컴퓨터단층혈관조영술은 컴퓨터작업(Rapidia, Infinitt)을 통하여 진행되었다. 자기공명혈관조영술 변수는 숙임각(flip angle) 20도, 바탕질(matrix) 수 320×224, 영상시야(field of view) 200× 200이었으며, 유체속도강조(Time-of-flight)기법으로 시행하였다. 삼차원자기공명혈관조영술은 대동맥부터 두개골중심 부위까지 재건하였다.
경동맥초음파촬영술과 뇌혈관조영술(컴퓨터단층혈관조영술 또는 자기공명혈관조영술)에서 보이는 혈관협착이나 폐색은 ‘있다’ 또는 ‘없다’로 판독하였다. 컴퓨터단층혈관조영술 또는 자기공명혈관조영술은 신경영상의학과 의사가 판독하였으며, 경동맥초음파촬영술은 신경과 의사가 판독하였다. 뇌혈관검사에서 관찰되는 기타 혈관부위의 협착소견(두개내혈관의 경우 50% 이상 협착, 두개외혈관의 경우 30% 이상) 유무도 확인하였다. 척추동맥기시부협착을 진단하는 두 가지 방법의 결과를 비교하였다. 또한 두 결과가 불일치할 경우에 그와 연관된 인자가 있는지 조사하였다.
결 과
2010년 3월에서 2011년 6월까지 총 482명의 환자가 경동맥초음파촬영술을 받았다. 그러나 137명에서만 양측 척추동맥기시부를 B모드영상에서 관찰할 수 있었다. 그들 중 73명이 뇌혈관조영술, 즉 자기공명혈관조영술 또는 컴퓨터단층혈관조영술을 받았다. 자기공명혈관조영술은 10명에서 시행되었고, 나머지는 컴퓨터단층혈관조영술을 받았다. 따라서 본 연구에서 73명을 최종 분석하였다.
남자는 46명으로 63%였으며 전체 환자의 평균연령은 61.05±11.90 (SD)였다. 대상환자들의 가장 흔한 진단은 허혈뇌졸중이었으며 전체 환자의 93.2% (68명)였다. 나머지 5명은 어지럼과 두통으로 병원에 와서 검사를 하게 된 환자였다.
오른쪽 척추동맥의 경우, 뇌혈관조영술 결과 22명에서 협착 및 폐색을 관찰하였다. 그러나 경동맥초음파촬영술에서는 그중 6명만이 협착 및 폐색소견을 보였다. 반대로, 뇌혈관조영술에서 협착 및 폐색이 없었던 두 명의 환자에서, 경동맥초음파촬영술에서 추가로 동맥경화판을 관찰할 수 있었다(Table 1, Fig.).
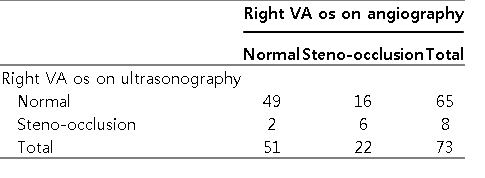
The comparison of the results of right vertebral arterial origin on CTA or MRA versus carotid ultrasonography
Computed tomography angiography of a 50 year-old man with pontine infarction shows stenosis of the left vertebral arterial origin (A, arrow). However, there was no stenosis on carotid ultrasonography (B). In 68-year-old woman with patent vessels on magnetic resonance angiography (C, arrow), atherosclerotic plaque was observed on carotid ultrasonography (D).
왼쪽 척추동맥의 경우, 16명에서 뇌혈관조영술에서 협착 및 폐색을 관찰하였으나 그 중 4명에서만이 경동맥초음파촬영술에서도 일치하는 협착소견이 있었다. 반대로 뇌혈관조영술에서는 정상소견을 보인 한 환자에서는 동맥경화에 의한 협착이 경동맥초음파촬영술에서 추가로 관찰되었다(Table 2, Fig.).
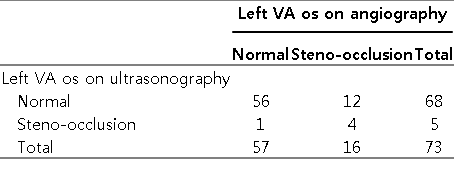
The comparison of the results of left vertebral arterial origin on CTA or MRA versus carotid ultrasonography
뇌혈관조영술에서 협착 및 폐색이 있었으나 경동맥초음파촬영술에서 정상을 보인 환자는각각 전체 73명 환자 중 21.9% (16명, 오른쪽), 16.4% (12명, 왼쪽)였다.
두 검사법의 결과가 일치하는 경우가 왼쪽 척추동맥의 경우, 총 73명 중 60명 즉 82.2%, 오른쪽 척추동맥의 경우 총 73명 중 55명 즉 75.3%였다.
뇌혈관조영술에서 오른쪽 또는 왼쪽 척추동맥기시부협착의 위양성을 보인 환자군과 그렇지 않은 군을 비교하였을 때, 고혈압, 당뇨병, 고지혈증과 같은 임상변수의 유의한 차이는 보이지 않았다. 기타 혈관의 협착소견도 양 군에서 유의한 차이가 없었다(Table 3).
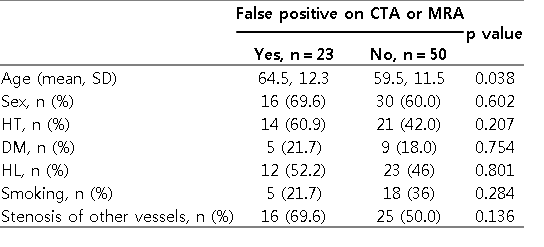
The factors related to the false-positive results of right or left vertebral artery origin on CTA or MRA versus carotid ultrasonography
고 찰
본 연구를 통하여 컴퓨터단층혈관조영술 및 자기공명혈관조영술에서 관찰된 척추동맥기시부협착 소견이 경동맥초음파촬영술에서는 관찰되지 않는 위양성 소견인 경우를 확인할 수 있었다. 반대로 뇌혈관조영술에서 정상으로 보였던 척추동맥기시부가 경동맥초음파촬영술에서 플라크에 의한 협착소견이 있는 것으로 관찰되기도 하였다.
컴퓨터단층혈관조영술과 초음파촬영술로 척추동맥을 평가한 결과에 대한 기존 문헌들이 있다. 한 연구는 척추동맥기시부에 중점을 두지 않았고, 또 다른 연구는 50% 이상 협착을 보인 경우만을 평가하였다[4,5]. 초음파촬영술로 검사했을 경우 척추동맥협착을 진단하는 민감도는 낮았으나 특이도는 높았다. 기존 연구들은 대상환자 수가 적었고, 디지털감산혈관조영술을 표준으로 비교하였다[5].
두 검사결과가 일치하지 않는 이유는 몇 가지로 설명이 가능하다. 두 검사법이 시행되는 시간적인 차이가 있기 때문에 다음 검사가 시작되기 전 혈관의 협착이 호전되거나 악화되는 변화를 보일 수 있다. 뇌혈관조영술에서 협착이 있으나 초음파촬영술에서 정상일 경우 혈관이 개통되었거나 척추동맥의 흐름허상에 의한 현상일 수 있다. 척추동맥기시부는 컴퓨터단층혈관조영술에서 위협착 소견을 잘 보이는 곳으로 알려져 있다. 체계적분석 논문에서 컴퓨터단층혈관조영술은 척추동맥기시부협착을 발견하는데 민감한 검사법이라고 하였으나, 본 연구와 함께 본다면 높은 위양성률도 가지고 있다고 볼 수 있겠다[6,7].
컴퓨터단층혈관촬영술에서 관찰되지 않던 죽경화판이 초음파촬영술에서 관찰되는 이유는 컴퓨터단층혈관촬영술은 혈관벽을 제외한 혈관내열림 상태만을 보여주기 때문이다[8]. 이러한 면에서 볼 때 경동맥초음파촬영술은 척추동맥경화판을 찾는데 있어 뇌혈관조영술에 비하여 장점이 있다. 그러나 척추동맥기시부는 깊숙이 존재하는 쇄골하동맥에서 분지하기 때문에, 좋은 음향창을 가지고 초음파를 투과시키는데 한계가 있다. 따라서, 뇌혈관협착을 진단하는데 있어 디지털감산혈관조영술이 표준이라는 것은 의심의 여지가 없다. 그러나 침습검사이기 때문에 모든 환자에게 안전하게 시행하기 어려운 단점이 있다. 또한, 혈관의 중첩과 꼬임에 의해 위음성 소견을 보일 수 있어 진단에 어려움을 겪은 보고도 있었다[9]. 따라서 실제 임상에서는, 컴퓨터단층혈관조영술 및 자기공명혈관조영술이 경동맥초음파촬영술과 함께 상호보완적으로 사용될 수 있을 것이다. 척추동맥기시부협착을 진단하는데 있어 경동맥초음파촬영술 적용의 제한점도 있다. 기존 연구결과를 본다면 척추동맥기시부 검사가 가능한 경우가 오른쪽의 경우 24.6%, 왼쪽의 경우 31.1%에 불과하였다고 한다[3]. 본 연구에서는 양쪽 척추동맥기시부가 모두 보인 경우가 28.4%(482명 중137명)였다. 본 연구에서는 양쪽 척추동맥이 모두 관찰된 경우를 등록하였다.
본 연구의 첫 번째 제한점은 척추동맥기시부의 플라크로 인한 협착을 초음파촬영술을 통하여 진단할 때에, 대부분 B모드영상을 이용하였으며, 속도기준을 적용하는데 한계가 있었다는 점이다. 따라서, 척추동맥협착의 정도 및 혈류역학적 관계를 충분히 고려한 결과가 아니다. 그러나, 척추동맥협착의 경우 속도기준에 대한 연구가 부족하고, 혈관의 비틀림과 혈류의 보상적 증가 가능성으로 인하여 협착을 진단하는 기준점(cut-off point)이 없는데, 이는 피할 수 없는 연구의 한계이다. 두 번째로 혈관협착 진단에 있어 최적 표준인 디지털감산혈관조영술을 시행하지 못하였다는 점이다. 이러한 점은 실제 임상과 동일한 경우를 재현하였다고도 볼 수 있으며, 컴퓨터단층혈관조영술 및 자기공명혈관조영술 또는 경동맥초음파촬영술, 두 검사법 중 어느 하나가 최적 표준이 될 수 없고 상호보완적으로 판단되어야 함을 강조하였다.