

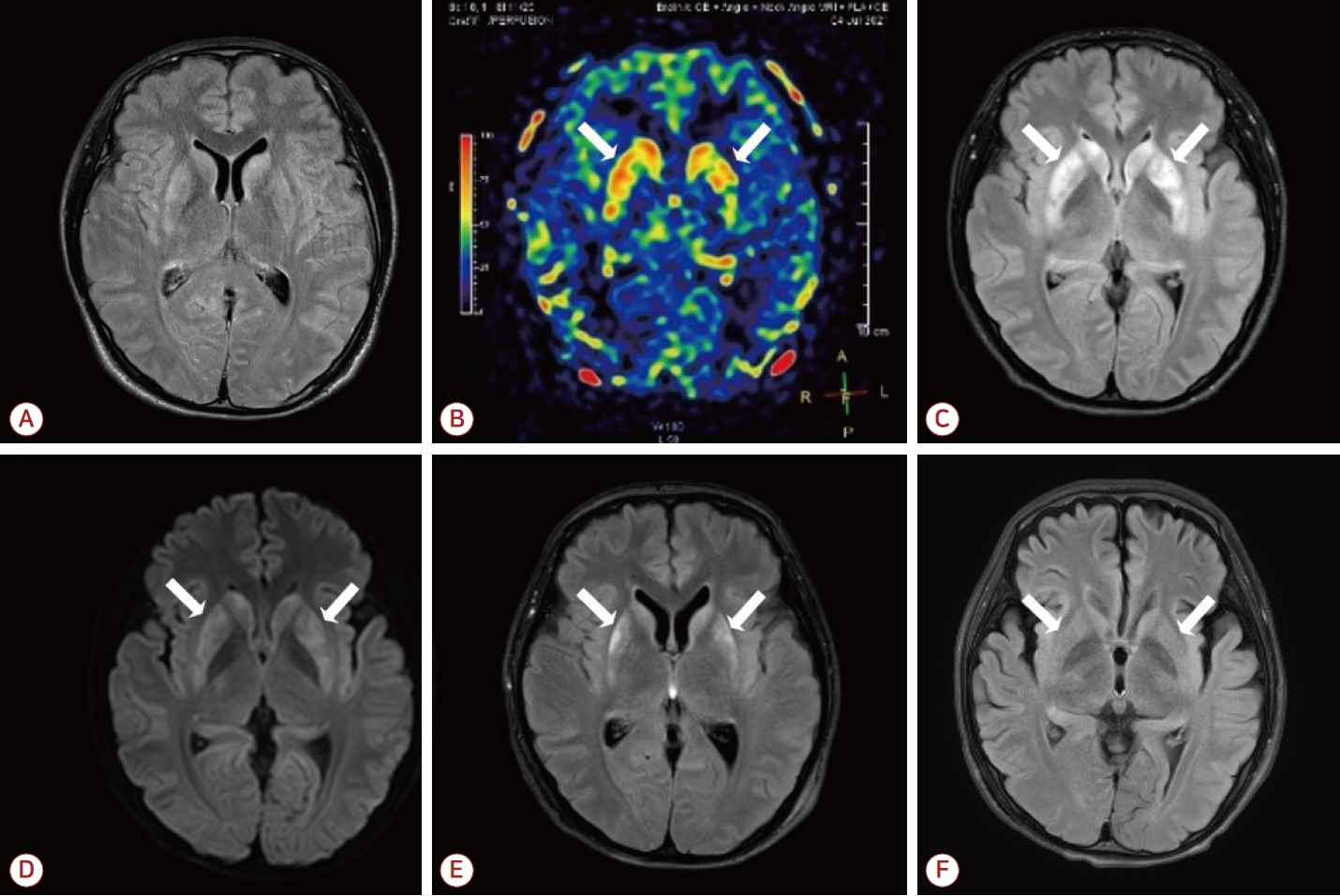
5일 전 설사, 발열 및 두통이 있었던 16세 남자가 전신강직간대발작과 혼미 상태로 내원하였다. 혈액 및 독성 검사에서 이상이 없었고, 뇌척수액 검사를 통해 감염뇌염을 배제하였다. 자가면역뇌염항체 검사는 음성이었고, 첫 뇌 자기공명영상(magnetic resonance imaging, MRI)에서 특이점이 없었으나(Fig. A), 동맥스핀 라벨링 관류 MRI에서 양측 꼬리핵과 조가비핵에서 혈류의 증가가 관찰되었다(Fig. B). 치료를 위해 레비티라세탐, 페니토인, 발프로산을 포함한 항뇌전증제와 프로포폴, 티오펜탈을 사용하였고, 1주 뒤 추적 관찰한 영상에서 선조체징후(striatal sign)를 보였다Fig. C, D). 선조체징후란 MRI에서 선조체에 고신호강도가 보이는 것을 의미하며, 전두엽이나 전측두엽에서 발생한 뇌전증지속상태를 진단하는 새로운 용어로 제안되었다[1]. 임상 양상에 근거해 열감염 관련 뇌전증증후군(febrile infectionrelated epilepsy syndrome, FIRES)으로 진단하여 스테로이드, 면역글로불린 및 리툭시맙 치료를 시작하였다. 3개월 후 영상 검사에서 호전을 보였고(Fig. E, F), 대화가 가능할 정도로 의식도 명료해졌다. 2년이 지난 현재 학교를 다니며 운동을 할 정도로 호전되어 외래 추적 관찰 중이다. FIRES는 2010년도에 처음 제안된 신발현 난치성 뇌전증지속상태에 대한 용어 중 하나로, 주로 학동기에 발생하나[2] 최근 더 높은 연령에서 다양한 MRI 소견이 보고되고 있다[3]. 증례와 같이 가역선조체징후가 나타나는 경우, FIRES의 가능성을 고려하여 신속한 치료를 진행하는 것이 필요하다.
| J Korean Neurol Assoc > Volume 41(4); 2023 > Article |

|
Acknowledgements
The authors express thank to the patient for generously authorizing us to share his rare case.
REFERENCES
1. Toudou-Daouda M, Bentamra L, Aminou-Tassiou NR, Smadja L, Soumah D, Chausson N, et al. Diffusion-weighted imaging hyperintensity of the striatum or “striatum sign’’ in convulsive status epilepticus. Seizure 2022;103:23-25.


2. Van Baalen A, Hausler M, Boor R, Rohr A, Sperner J, Kurlemann G, et al. Febrile infection-related epilepsy syndrome (FIRES): a nonencephalitic encephalopathy in childhood. Epilepsia 2010;51:1323-1328.
3. Culleton S, Talenti G, Kaliakatsos M, Pujar S, D’Arco F. The spectrum of neuroimaging findings in febrile infection-related epilepsy syndrome (FIRES): a literature review. Epilepsia 2019;60:585-592.
Figure.
MRI change of the patient. (A) The patient’s initial T2-weighted FLAIR showed no abnormal signals. (B) However, the initial arterial spin labeling image showed hyperperfusion in the bilateral caudate nucleus and putamen (arrows). After 1 week, (C) T2-FLAIR and (D) diffusion- weighted imaging revealed symmetric hyperintensities in the same lesions with isointense signals on apparent diffusion coefficient sequence (not shown, arrows). After 1 month, (E) FLAIR hyperintensities on both striata (arrows) had decreased. After 3 months, (F) FLAIR signal change had almost completely recovered (arrows), showing a reversible striatal sign with additional bilateral frontal lobe atrophy as a sequela. MRI; magnetic resonance imaging, FLAIR; fluid-attenuated inversion recovery.
- TOOLS
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print


-
METRICS

-
- 0 Crossref
- 0 Scopus
- 192 View
- 12 Download
-

- Related articles
- Editorial Office
-
(ZIP 03163) #1111, Daeil Bldg, 12, Insadong-gil, Jongno-gu, Seoul, Korea
Tel: +82-2-737-6530 Fax: +82-2-737-6531 E-mail: jkna@neuro.or.kr
Copyright © 2024 by Korean Neurological Association.

