


서 론
혈관주위공간(perivascular space, PVS)은 뇌척수액으로 채워진 공간으로 뇌실질을 관통하는 소혈관을 둘러싸고 있다[1]. 이전에는 특별한 임상 의의를 가지지 않는 것으로 여겨졌으나 최근 글림프계(glymphatic system) 개념이 등장하면서 주목받게 되었다[2]. 글림프계는 신경아교세포(glia cell)와 림프계(lymphatic system)의 합성어로, 별아교세포(astrocyte)와 혈관벽세포로 이루어져 뇌척수액 순환을 통해 노폐물을 제거하는 림프계의 역할을 한다. 글림프계에서 PVS는 뇌척수액과 간질액 사이의 교환이 일어나는 통로로 뇌의 대사산물 제거에 중요한 역할을 할 것으로 여겨진다[3]. PVS는 현미경에서 관찰할 수 있는 구조물이나, 병적으로 늘어나게 되면 뇌 자기공명영상(magnetic resonance imaging, MRI)에서도 확인할 수 있게 되고 이를 확장된 혈관주위공간(enlarged PVS, ePVS)이라 부른다[4]. ePVS는 MRI에서 뇌척수액과 비슷한 신호 강도를 보이고, 주로 기저핵(basal ganglia, BG), 반난형백질중심부(centrum semi-ovale, CSO), 중뇌(midbrain), 해마(hippocampus), 측두엽 등에서 관찰할 수 있다[1,5,6].
PVS의 확장에 대해서는 몇 가지 가설이 존재한다. 첫째, 고혈압이나 동맥벽의 죽상경화로 인해 혈관벽이 손상되면서 혈관 투과성이 증가하여 세동맥 주변의 PVS 확장을 유발할 수 있다[7]. 둘째, 신경염증 반응으로 뇌혈관장벽(brain blood barrier)의 투과성이 증가하여 PVS가 확장된다[8]. 셋째, 베타-아밀로이드(β-amyloid, Aβ)가 혈관벽에 응집되어 아밀로이드 혈관 병증(cerebral amyloid angiopathy, CAA)이 발병하면, 축적된 Aβ가 PVS를 통한 액체 교환을 방해하여 ePVS를 유발한다. 이로 인해 대사산물의 제거 기능이 저하되면 결국 Aβ와 같은 노폐물 침착이 가속화되는 악순환을 반복한다는 가설이다[9]. 이러한 가설들을 바탕으로 최근 한 연구에서 ePVS는 백질 고신호강도(white matter hyperintensity, WMH), 뇌미세출혈(cerebral microbleed, CMB), 열공경색(lacune)과 함께 뇌소혈관 질환의 영상 표지자 중 하나로 대두되고 있다[10]. 또한 알츠하이머병, 파킨슨병, 헌팅턴병 등의 신경퇴행 질환이나 뇌출혈, 뇌허혈과 같은 뇌혈관 질환, 다발경화증을 비롯한 신경염증 질환을 포함한 다양한 신경계 질환에서 ePVS와의 연관성에 대한 연구들이 진행되고 있다[11].
알츠하이머병은 전체 치매의 60-80%를 차지하는 신경퇴행 치매의 가장 흔한 원인으로 주요 병리는 신경세포 밖에 침착된 Aβ 단백으로 이루어진 아밀로이드판(amyloid plaques)과 타우(tau) 단백 이상에 의해 세포 안에 생기는 신경원섬유 매듭(neurofibrillary tangles)이다[12]. 앞서 언급한 PVS의 확장에 대한 가설 중 Aβ 관련 가설을 바탕으로 알츠하이머병과 ePVS 연관성에 관한 연구들이 발표되었다. 알츠하이머병 치매 환자와 정상 노인들을 대상으로 한 연구에서 기저핵의 ePVS (BG-ePVS)는 알츠하이머병 치매와 연관이 없었고, 백질반난형 중심의 ePVS (CSO-ePVS)는 알츠하이머병 치매와 유의한 연관성을 보였다[13]. 알츠하이머병 치매와 혈관인지장애 환자를 대상으로 한 연구에서도 CSO-ePVS는 알츠하이머병 치매와, BG-ePVS는 혈관인지장애와 유의한 연관성을 보고하였다[14]. 이후 아밀로이드 침착과 ePVS의 관련성을 확인하기 위하여 아밀로이드-양전자방출단층촬영(amyloid-positron emission tomography, amyloid-PET)과[15,16] 뇌척수액 생물표지자를 이용한 여러 연구들이 진행되었으나[17-19] 각기 상반된 연구 결과를 보고하였다.
ePVS와 인지 저하에 관해서도 많은 연구들이 시행되었으나 일관성 있는 결과를 보이지는 않았다. ePVS가 많을수록 인지기능이 저하된다는 보고들이 있었으나[20,21] 다른 연구에서는 유의한 연관성이 없었다[22]. 최근 발표된 국내 연구에서는 BG-ePVS가 많을수록 집행기능의 저하가 있었으나 뇌소혈관 질환의 지표를 통제하면 연관성이 사라졌다[23].
이에 본 연구는 다음과 같은 목표로 설계되었다. 첫째, 부산대학교병원에 통원 중인 신경퇴행 질환 환자들을 대상으로 질환별 ePVS의 분포와 정도를 파악하고, ePVS 분포에 따른 인지기능과의 연관성을 파악한다. 둘째, 아밀로이드 침착, 혈관 위험인자, 뇌소혈관 질환 표지자와 ePVS 분포와의 관련성을 확인한다. 그리고 ePVS 발생 가설과 기존 연구 결과를 바탕으로 ePVS는 인지장애가 심할수록 그 정도가 심하고, CSO-ePVS는 알츠하이머병 치매, 아밀로이드 침착과 연관이 있으며, BG-ePVS는 혈관위험인자, 뇌소혈관 질환 표지자와 관련이 있을 것으로 예상하였다.
대상과 방법
1. 대상
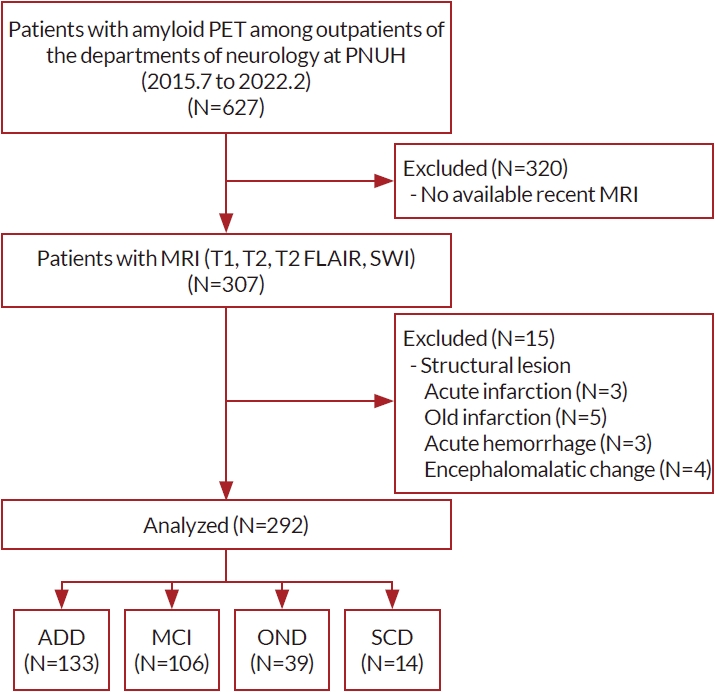
2015년 7월부터 2022년 2월까지 부산대학교병원 신경과 인지장애 클리닉에 내원하여 amyloid-PET과 뇌 MRI를 시행한 307명의 환자 중 뇌경색, 뇌출혈 등 광범위한 구조적 이상이 동반된 15명을 제외한 총 292명의 환자를 연구 대상자로 하였다. 모든 연구 대상자에서 신경과 의사에 의한 임상 면담, 신경계진찰, 인지기능 평가, 혈액 검사가 시행되었다. 임상 진단명에 따라 알츠하이머병 치매[24], 경도인지장애[25,26], 기타 신경퇴행 질환, 주관 인지 저하[27]의 네 그룹으로 구분하였고, 기타 신경퇴행 질환에는 전두측두엽 치매[28], 레비소체 치매[29], 파킨슨병[30], 비정형파킨슨증[31-33], 척수소뇌실조, 백질형성장애를 포함하였다(Fig. 1).
2. 뇌 MRI
뇌 MRI는 3-T MR Scanner (Verio, Skyra Ⅰ or Ⅱ, MAGNETOM Trio A tim; Siemens, München, Germany)를 이용하여 획득하였다. 모든 대상자에서 3D T1 강조영상, T2 강조영상을 포함하였고, T2 강조영상의 화소 배열 수(matrix size)는 358×512였다. 268명에서 액체감쇄회복역전영상(fluid-attenuated inversion recovery, FLAIR)을 포함하였는데 209명에서 절편 두께 2 mm, 59명에서 절편 두께 5 mm로 시행하였다. 286명에서 자화율강조영상(susceptibility-weighted image, SWI)을 포함한 영상을 획득하였다.
3. ePVS 측정
ePVS는 standards for reporting vascular changes on neuroimaging (STRIVE)에 제시된 방법에 따라 MRI T2 강조영상에서 고신호강도를 보이는 3 mm 이하의 작고 둥근, 혹은 길쭉한 선형의 경계가 좋은 병변으로 정의하였다[34]. BG-ePVS는 앞맞교차(anterior commissure)의 바로 위 단면에서 측정하고 좌우측 개수를 따로 세어 평균을 구하였다[35]. CSO-ePVS는 가쪽뇌실(lateral ventricle)의 바로 위 단면에서 측정하고 좌우측 개수를 따로 세어 평균을 구하였다[36]. ePVS의 수는 좌우측 중 개수가 많은 쪽의 수에 따라 5점 척도(0, 0 PVS; 1, ≤10 PVS; 2, 11-20 PVS; 3, 21-40 PVS; 4, >40 PVS)로 구분하고[10], 이를 바탕으로 두 단계(낮은 단계, 5점 척도 0-1; 높은 단계, 5점 척도 2-4)로 나누어 분석하였다(Fig. 2).
4. 대뇌소혈관 질환 지표 측정
열공경색은 STRIVE에 따라 뇌척수액과 비슷한 신호 강도를 보이는 3 mm에서 15 mm 크기의 둥글거나 타원형 또는 관 모양의 공동성 병변으로 정의하였다[34]. T2 FLAIR 영상에서 병변의 중심부는 저신호강도를 보이고 테두리는 고신호강도를 보이는 특징이 있다. ePVS와 비교하여, 테두리 고신호강도를 보이면서 3 mm보다 큰 경우는 열공경색으로 판단하였다[37]. 대뇌피질, 피질하백질, 심부뇌회백질핵(기저핵, 시상), 뇌간, 소뇌로 위치를 나누어 개수를 세었다. 뇌미세출혈은 Greenberg 기준에 따라 SWI에서 신호 소실을 보이는 원형 또는 타원형 병변 중 직경이 10 mm 이하인 것으로 측정하였고[38], 열공경색과 마찬가지로 대뇌피질, 피질하백질, 심부뇌회백질핵(기저핵, 시상), 뇌간, 소뇌로 위치를 나누어 개수를 세었다. 백질 고신호강도는 STRIVE에 따라 절편 두께 2 mm T2 FLAIR 영상에서 신호가 증가된 백질 부위로 정의하였고[34], Statistical Parametric Mapping (SPM, https://www.fil.ion.ucl.ac.uk/spm/) 패키지인 Lesion Segmentation Tool로 추출하고 Advanced Normalization Tools로 표준화하여 voxel-based morphometry로 용적을 측정하였다[39].
5. Amyloid-PET 획득과 분석
모든 대상자는 18F-flumtemetamol 혹은 18F-florbetaben amyloid-PET를 시행하였다. PET는 환자의 임상 정보를 모르는 핵의학전문의가 시각적으로 평가하여 아밀로이드 양성, 음성으로 구분하였다. 아밀로이드 음성은 피질하백질의 비특이적 방사능 섭취가 있고 뇌피질에는 섭취가 거의 없어 피질하백질과 뇌피질의 대조가 선명한 경우로 정의하였고, 아밀로이드 양성은 뇌피질에서의 방사능 섭취가 주변 피질하백질과 비교하여 높거나 비슷하여 백질과 피질의 경계가 불분명한 경우로 정의하였다[40].
6. 인지기능 평가
289명의 환자에서 간이 정신상태 검사(mini-mental state examination, MMSE)를 시행하였고 252명의 환자에서 서울 신경심리선별 종합 검사(Seoul Neuropsychological Screening Battery, SNSB)를 시행하였다[41]. 인지 기능은 주의집중능력(숫자 바로 따라 외우기[digit span test-forward, DST-F], 숫자 거꾸로 따라 외우기[digit span test-backward, DST-B]), 언어기능(이해하기, 따라 말하기, 한국판 보스톤 이름대기 검사[Korean-Boston naming test, K-BNT]), 시공간기능(시계 그리기 검사[clock drawing test, CDT], 레이 복잡도형 검사[Rey-Osterrieth complex figure test, RCFT]), 기억력(서울 언어학습 검사[Seoul verbal learning test, SVLT], RCFT 즉각회상, 지연회상, 재인 검사), 전두엽/집행기능(go-no-go test, 연상단어구술 검사[controlled oral word association test, COWAT]의 음소유창성[phonemic fluency] 검사, 한국판 색단어간섭 검사[Korean-color word stroop test: color reading, K-CWST: CR], 숫자-기호 바꿔쓰기 검사[digit symbol coding, DSC], 한국판 노인형 기호잇기 검사 part B [Korean version of trail making test for elderly person part B, K-TMT-E part B])의 5가지 영역으로 나누어 평가하였고, 각 인지 영역의 z-score를 비교하였다[42]. 그리고 285명의 환자에서 임상치매 평가 척도(clinical dementia rating scale, CDR)를 측정하여 치매의 중등도를 평가하였다.
7. 통계
임상 진단 그룹 간 인구학적 특징, ePVS 정도, 대뇌소혈관 지표, 아밀로이드 PET 양성/음성 여부, 인지기능을 비교하였다. 연속형 변수일 경우 Kruskal-Wallis 분석으로 비교하였고 범주형 변수일 경우 chi-square/Fisher’s exact test를 이용하여 비교하였다. ePVS와 인지영역 z-score와 MMSE 총 점과의 관련성은 성별, 연령, 교육 수준, 임상 진단을 통제한 일반 선형 모델을 적용하였다. ePVS와 아밀로이드 침착, 혈관 위험인자, 뇌소혈관 질환 표지자와의 관련성은 ePVS를 낮은 그룹과 높은 그룹으로 나누어 이분형 로지스틱 회귀를 이용하여 분석하였다. ePVS의 아밀로이드 병리 예측 가능성을 확인하기 위하여 전체 대상자를 amyloid-PET 양성군과 음성군으로 나누었고, 두 집단의 인구학적 특징은 연속형 변수일 경우 Mann-Whitney U test를 이용하여 비교하였다. 그리고 Amyloid-PET 양성을 종속변수로, BG-ePVS와 CSO-ePVS 각각을 독립변수로 하여 로지스틱 회귀 분석을 시행하였다. 이때 연령, 성별, APOE E4 유전자 유무, 백질변성용적, 진단 그룹을 통제하였다. 다중 검정에 대한 보정은 Bonferroni 방법과 false discovery rate (FDR) 방법으로 수정하였다.
결 과
1. 인구학적 특징과 ePVS의 분포와 정도
최종 연구 대상 292명 중 133명이 알츠하이머병 치매, 106명이 경도인지장애, 39명이 기타 신경퇴행 질환 환자, 14명이 주관 인지 저하였다. 나이는 알츠하이머병 치매군이 기타 신경퇴행 질환군에 비해 많았고 발병 연령은 알츠하이머병 치매군과 경도인지장애군에서 기타 신경퇴행 질환군에 비해 높았다. 성별과 교육 수준은 네 군에서 통계적으로 유의한 차이가 없었다. APOE E4 유전자는 알츠하이머병 치매군에서 유의하게 많았다. Amyloid-PET의 시각적 평가를 통해 아밀로이드 침착을 비교하였을 때 알츠하이머병 치매군에서 다른 세 군에 비해 아밀로이드 양성이 많았다. 알츠하이머병 치매군과 기타 신경퇴행 질환군에서 경도인지장애군과 주관 인지 저하군에 비하여 MMSE, 5가지 인지영역별 z-score는 낮았고 CDR은 높았다. 고혈압, 당뇨는 네 군에서 통계적으로 유의한 차이가 없었으나 주관 인지 저하군에서 고지혈증을 가진 비율이 높았다. 열공경색과 뇌미세출혈은 네 군에서 유의한 차이가 없었으나 백질변성용적은 알츠하이머병 치매군이 경도인지장애군보다 많았다. 네 군에서 BG-ePVS와 CSO-ePVS 모두 평균 개수에서 유의한 차이가 없었고 두 단계(낮은 단계, 높은 단계)로 분류했을 때도 분포의 차이를 보이지 않았다(Table 1).
2. ePVS 분포에 따른 인지기능과의 연관성
ePVS와 인지기능과의 연관성을 알아보기 위해 일반 선형 모델을 적용하였다. 높은 단계의 BG-ePVS는 MMSE, 5가지 인지영역 지표와 유의한 연관이 없었다. CSO-ePVS는 시공간 기능과 연관이 있었으나, FDR 보정을 시행하면 연관성이 사라졌고 나머지 인지기능 지표와도 유의한 연관이 없었다(Table 2).
3. 뇌소혈관 질환 지표, 혈관위험인자, 아밀로이드 침착과 ePVS 분포와 정도의 관련성
뇌소혈관 질환 지표(열공경색, 뇌미세출혈, 백질변성용적), 혈관위험인자(당뇨, 고혈압, 고지혈증), 아밀로이드 침착 유무를 각각 독립변수로 두고, ePVS 단계를 종속변수로 하여 로지스틱 회귀 분석을 시행하였다. 이때 연령, 성별, APOE E4 유전자 유무를 통제하였다. BG-ePVS는 열공경색이 있을수록 높은 단계와 관련이 있었고, 아밀로이드 침착이 있을수록 낮은 단계와 관련이 있었다. 하지만 CSO-ePVS와 유의한 연관성을 보이는 뇌소혈관 질환 지표와 혈관위험인자는 없었고, 아밀로이드 침착 유무와도 관련이 없었다(Table 3).
4. ePVS와 아밀로이드 병리
총 292명 중 127명이 아밀로이드 음성이었고 165명이 아밀로이드 양성이었다. 연령, 성별, 발병 연령, 교육 수준에는 유의한 차이가 없었고 아밀로이드 양성군에서 APOE E4 유전자와 알츠하이머병 치매 환자가 많았다. 아밀로이드 양성군에서 MMSE 점수가 유의하게 낮았으며 CDR 점수는 더 높았다. 기억력은 아밀로이드 양성군이 음성군에 비해 저하되어 있었으나 그 외 다른 인지영역 평가에서는 유의한 차이를 보이지 않았다. 당뇨 유병률은 아밀로이드 음성군에서 더 높았고 열공경색도 음성군에서 더 많았다. 뇌미세출혈과 백질변성용적에서는 유의한 차이가 없었다. ePVS의 분포를 비교하였을 때, 아밀로이드 음성군에서 양성군에 비해 BG-ePVS의 평균값이 높았고 높은 단계의 BG-ePVS가 더 많았으나, CSO-ePVS는 두 군에서 유의한 차이가 없었다(Table 4). 로지스틱 회귀 분석 결과, CSO-ePVS가 높은 단계일수록 아밀로이드 양성을 예측할 수 있었고(odd ration [OR], 2.351; 95% confidence interval [CI], 1.162-4.759; p=0.017), BG-ePVS가 높은 단계일수록 아밀로이드 양성의 확률은 떨어졌다(OR, 0.336; 95% CI, 0.158-0.715; p=0.005) (Table 5).
고 찰
본 연구 결과를 정리하면 다음과 같다. 첫째, 알츠하이머병 치매, 경도인지장애, 기타 신경퇴행 질환, 주관 인지 저하에서 ePVS의 정도와 분포에는 차이가 없었다. 둘째, BG-ePVS와 CSO-ePVS 모두 인지기능과 연관이 없었다. 셋째, 열공경색이 있을수록 높은 단계의 BG-ePVS가 예측되고, 아밀로이드 양성의 경우 높은 단계의 BG-ePVS 가능성이 떨어진다. 넷째, 아밀로이드 음성군은 양성군에 비해 높은 단계의 BG-ePVS, 당뇨, 열공경색의 빈도가 높았고, 높은 단계의 CSO-ePVS일수록 아밀로이드 양성일 확률이 높았으며, 높은 단계의 BGePVS일수록 아밀로이드 양성일 확률은 낮았다.
ePVS와 인지기능의 연관성을 조사한 선행 연구 결과들은 서로 일치하지 않는 결과를 보인다. 5개의 일반인구 기반 연구 결과를 정리한 메타 연구에 의하면, ePVS의 총 개수와 인지기능 간 유의한 상관은 없었고, 중뇌, 기저핵, 해마, 반난형백질중심부로 나누어 측정한 각 뇌영역별 ePVS 수와도 인지기능은 상관이 없었다[22]. 정상인과 경도인지장애 환자들을 대상으로 한 연구는 BG-ePVS 수가 많을수록 정보 처리 속도, 집행기능, 시공간기능의 악화를 보고하였다[43]. 국내에서 진행된 amyloid-PET 양성의 알츠하이머 연속체(알츠하이머병 치매와 임상 전단계)에 해당하는 환자를 대상으로 한 연구와[44] 다양한 진단(주관인지장애, 경도인지장애, 알츠하이머병 치매, 혈관 치매와 혼합 치매, 기타 치매)을 가진 대규모 환자를 대상으로 한 연구에서는 BG-ePVS는 전두엽/집행기능과 관련이 있었으나 뇌소혈관 질환 지표를 통제하면 그 유의성은 사라졌고, CSO-ePVS는 공변량과 상관없이 인지기능과의 유의한 연관성이 없었다[23]. 이처럼 ePVS와 인지기능의 연관성에 대한 이전의 연구에서 상반된 결과를 보고하나, 최근 대다수 연구에서 CSO-ePVS는 인지 저하와 관련이 없고, BG-ePVS의 경우 전두엽/집행기능의 저하와 관련이 있다고 보고하고 있다. 본 연구에서 BG-ePVS와 CSO-ePVS의 높은 단계는 5가지 인지 영역과 MMSE, CDR과 연관이 없었다. 본 연구는 기존 연구에 비해 연구 대상자가 적고, 비슷한 연구 대상자 수라도 높은 단계의 ePVS 대상자의 분포가 적은 점 등이 선행 연구 결과와의 차이를 유발하였을 것으로 추정한다[23,44].
본 연구에서는 뇌소혈관 질환 지표 중의 하나인 열공경색이 있을수록 BG-ePVS가 많았다. 이는 BG-ePVS가 혈관인지장애와 연관이 있다는 이전 연구 결과와 부합하며[14] 뇌소혈관 질환과 BG-ePVS가 공통된 병리를 공유함을 시사한다. CSO-ePVS는 혈관위험인자와 뇌소혈관 질환 지표와 연관이 없는 반면, amyloid-PET 양성의 독립적인 예측 인자였다. 높은 단계의 CSO-ePVS를 보일 때 amyloid-PET 양성일 가능성이 높았고 이는 CSO-ePVS가 아밀로이드 병리와 연관되어 있음을 시사한다. 이전 연구들에서도 CSO-ePVS는 알츠하이머병 치매과 유의한 연관을 보였다[13,15]. Amyloid-PET을 이용하여 아밀로이드 침착과 CSO-ePVS의 연관성을 확인하는 기존의 연구들에서 상반된 결과가 보고되기도 하였는데 이러한 연구들은 본 연구와 대상군에 차이가 있었다[14,17]. 본 연구는 주관 인지 저하와 경도인지장애뿐 아니라 알츠하이머병 치매와 다른 신경퇴행 질환 환자들을 포함하여 다양한 정도의 인지를 가진 환자들을 대상으로 하였으며, ePVS 측정에 영향을 줄 수 있는 뇌경색이나 뇌출혈 등 큰 구조적 병변을 가진 환자들은 제외하였다. 혈관 치매 환자들을 다수 포함한 연구에서는 구조적 병변으로 인해 정확한 ePVS 측정에 영향을 받았을 수 있다[14]. 인지 정상군과 경도인지장애와 같이 비교적 인지 저하가 심하지 않은 환자를 대상으로 한 연구에서 CSO-ePVS와 amyloid-PET 양성이 연관이 없다는 결론을 얻었으나 이는 초기 인지 저하 환자를 대상으로 한 연구로 본 연구의 대상자와 인지 저하의 정도에 차이가 있었다[17]. 알츠하이머병 치매와 경도인지장애를 대상으로 한 국내 연구에서는 본 연구와 동일한 결과를 보였다[15].
본 연구의 제한점은 다음과 같다. 첫째, 표본의 크기가 작다. 주관 인지 저하에서 알츠하이머병 치매까지 인지 저하의 정도가 다양한 환자들을 포함하였으나 전체 대상자가 292명으로 표본 수가 충분하지 않았으며 주관 인지 저하 환자는 14명만 포함되었다. 둘째, ePVS와 뇌소혈관 질환을 측정할 때 정량 분석이 아닌 시각적 평가를 시행하였고, 특히 열공경색 측정에 절편의 두께가 다른 영상을 같이 활용하여 측정의 정확도에 제한점이 있다. 하지만 ePVS 측정 시 교육과 반복적인 측정을 통해 시각적 평가 간 일치율을 높이고자 하였고, 열공경색은 유무로만 분석하여 절편 두께가 다름으로 인해 발생할 수 있는 병변 개수 차이를 최소화하고자 하였다. 그러나 향후 정량 분석을 적용한 연구들이 필요하다. 셋째, ePVS를 단 하나의 단면에서만 측정하여 실제 개수보다 적게 측정되었을 가능성이 있다. 하지만 한 개의 단면에서 측정한 값과 전체 단면에서 측정한 값 사이에 높은 상관관계를 제시한 기존 연구가 존재한다[45]. 넷째, 아밀로이드 침착을 확인할 때 amyloid-PET를 통한 비교만 시행하였다. Amyloid-PET보다 뇌척수액 생물표지자가 뇌조직의 아밀로이드 침착을 더 민감하게 반영한다는 보고가 있었다[46]. 따라서 아밀로이드 병리와의 연관성을 확인하기 위해서 뇌척수액 생물표지자 등을 통한 분석도 추가적으로 필요하다. 다섯째, 본 연구에서는 ePVS의 분석을 CSO와 BG 두 곳만으로 한정하였으나 최근에는 해마와 중뇌의 ePVS를 함께 분석하여 뇌영역별 ePVS의 특징을 분석하는 경향이 있다[5,22]. 특히 인지기능과의 연관성을 관찰한 연구에서 해마 ePVS와 기억력과의 연관성을 보고하기도 하였으나, 본 연구에서는 해마 ePVS 분석이 이루어지지 않아 선행 연구 결과를 확인할 수 없었다.
결과적으로 본 연구 결과는 ePVS가 뇌영역의 분포에 따라 다른 기저 병리를 가진다는 가설을 뒷받침한다. 즉 BG-ePVS는 뇌소혈관 질환과 혈관위험인자와 관련성으로 미루어 보아 혈압 관련 동맥 병증에 기인하고, CSO-ePVS는 아밀로이드 병리와의 관련성으로 미루어 보아 CAA에 기인되었을 가능성을 추정해 볼 수 있다.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




