임상추론: 기침 후 벼락두통으로 내원한 28세 남자
Clinical Reasoning: A 28-Year-Old Male Presenting with Cough induced Thunderclap Headache
Article information
증 례
특이병력 없는 28세 남자가 내원 3주 전부터 시작된 수치통증척도(numeric rating scale) 9/10점의 앞머리 전체가 터질 듯한 심한 두통으로 내원하였다. 내원하기 전 총 3번의 같은 양상의 두통이 발생했는데, 3번의 두통 모두 1분 이내에 최대 강도에 도달하였고, 20분가량 지속되었다. 기침을 할 때 두통이 발생했고, 기침을 할 때와 변을 보면서 배에 힘을 줄 때 악화되었다. 구역과 구토는 동반되었으나 빛공포증과 소리공포증은 없었고 시야장애와 시력저하 또한 없었다. 환자는 처음 겪는 두통이고 음주, 흡연은 하지 않았고, 복용하는 약물도 없었으며, 최근 외상병력도 없었다.
내원 당시 활력징후는 혈압은 130/90 mmHg였고, 발열은 없었다. 신경계 진찰에서 의식은 명료하고, 동공반사 및 안구운동은 정상이었고, 경부강직도 없었다.
입원하여 내원 1일에 뇌 혈관전산화단층촬영(computed tomography angiography, CTA)을 시행하였고, 그 후 시행한 뇌척수액검사는 정상이었으며, 일반혈액검사, 일반화학검사, 적혈구침강속도, 갑상선기능검사, 항핵항체검사, 류마티스인자, 루푸스항응고인자, 항카디오리핀항체, 항 beta2 glycoprotein 1 항체도 모두 정상이었다.
질문 1. 증상 초기 진단을 위해 고려해야 하는 것들은 무엇인가?
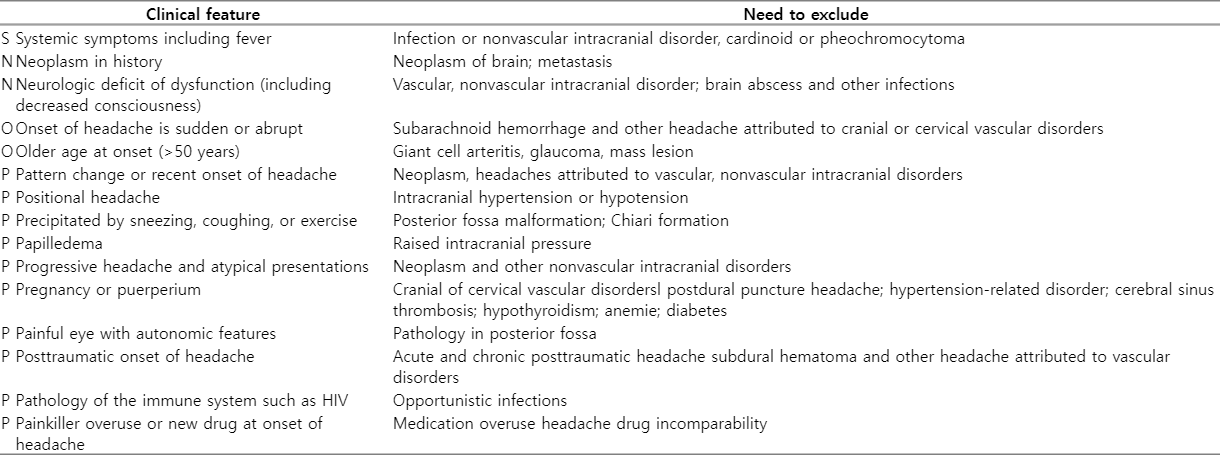
두통 환자를 진단할 때 가장 중요하고 먼저 해야 할 것은 정확한 병력을 청취하는 것이다. 이를 통해 심각한 두통이 있다면 진단검사나 영상검사를 통해 이차두통이 있는지 감별할 수 있다. 병력상 이차두통을 감별할 수 있는 SNNOOP10 (Table 1) 중 이 환자에서는 경험하지 못한 심한 새로운 두통, 갑자기 발생한 벼락 두통, 발살바수기와 기침 시 악화라는 적신호(red flag)를 가지고 있는 점에서 이차두통의 가능성을 두고 적절한 검사를 계획하고 시행하여야 한다. 이차두통이 있는 환자에서는 신경학적 증상의 동반 여부, 의식변화, 수막자극증상, 시신경유두부종, 시야 장애 양상, 두부외상이나 두피상처 여부, 경동맥 잡음, 안와 잡음, 측두동맥의 압통 여부, 발열 여부 등을 반드시 관찰하여야 한다. 이 환자에서는 초기 신경계 진찰에서 뇌압상승 여부를 확인하지 않았지만, 항상 이차두통이 의심이 된다면, 시신경유두부종 같은 뇌압상승 징후를 항상 확인하는 것이 필요하다. 두통의 원인이 되는 이차적인 문제가 없다고 확인할 때까지 일차두통의 가능성도 염두하고 국제두통질환분류(international Classification of Headache disorder, ICHD)의 진단기준에 맞추어 진단한다[1].
질문 2. 이 환자의 두통으로 감별할 수 있는 진단은 무엇인가?
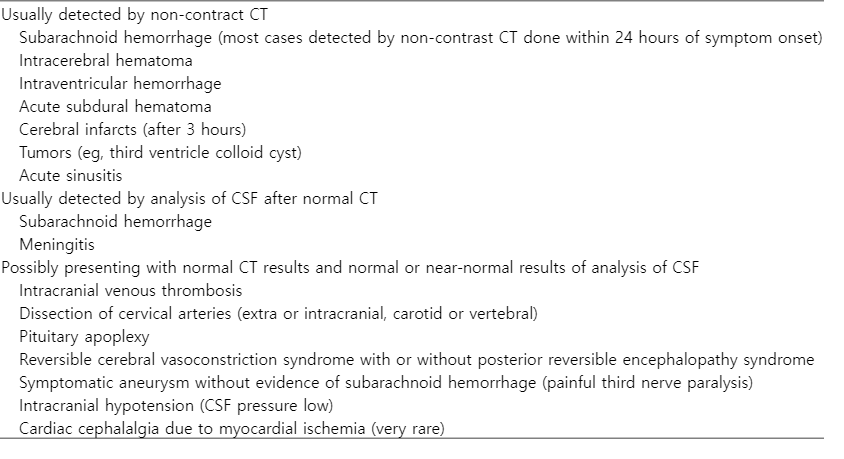
벼락두통은 보통 1분 이내에 통증이 최고조에 이르고 이제까지 경험하지 못한 강도로 심한 두통을 말한다. 주로 갑자기 깨질 듯이, 망치로 내려치듯이 아프다고 말하기도 하며 생명을 위협할 수 있거나 장애를 일으키는 이차두통의 발현증상으로 나타나므로 감별 진단이 중요하다(Table 2) [2].
여러 뇌혈관질환이나 두개내 이상이 벼락두통의 원인이 될 수 있다. 특히 거미막하출혈, 가역뇌혈관수축증후군(reversible vasoconstriction syndrome, RCVS), 뇌동맥박리, 뇌정맥혈전증은 드물지 않게 발현되기 때문에 중요한 감별진단이다. 특정 유발요인이 있는 경우 일차운동두통, 일차성행위연관두통, 일차기침두통 등으로 분류하고, 이에 맞지 않는 벼락두통은 일차벼락두통으로 분류하는데, 임상적으로 벼락두통을 호소하는 모든 환자들에게는 이차두통을 배제하기 위한 검사를 시행하도록 권고해야 한다.
질문 3. 이 환자에게 다음으로 시행할 수 있는 적절한 검사는?
환자는 내원 전까지 극심한 벼락두통을 3번 호소하였다. 초기 뇌 computed tomography (CT)는 정상이고 발열이 없고, 수막자극 증상은 없었기 때문에 종양 같은 뇌공간점유병소질환, 거미막하출혈, 뇌출혈, 뇌경색 등은 배제할 수 있다. 하지만, 키아리 기형, 뇌하수체의 질환, RCVS, 뇌동맥 박리 등은 뇌 CT로 감별이 어렵기 때문에 CTA나 자기공명영상(magnetic resonance imaging, MRI) 및 자기공명 혈관조영(magnetic resonance angiography, MRA) 가 필수적이다. 만약 CTA와 MRA에서 문제가 발견되지 않았다면 뇌압 상승 여부를 위해 뇌척수액 검사를 통해 뇌척수액 압력을 확인하여 다른 동반질환이 있는지 확인해야 한다.
이 환자에서는 내원 1일째 CTA에서 양쪽 전대뇌동맥의 A2와 왼쪽 A3 분절에 불규칙하게 다발성 수축이 발견되었다. CTA 촬영 다음 날에 환자는 기침두통 및 벼락두통이 재발하였고, 내원 7일째 시행한 MRA에서는 양쪽 A2분절의 불규칙한 혈관협착은 남아 있었으나 왼쪽 A3 분절의 협착은 사라졌고, 오른쪽 A2 분절의 혈관박리로 의심되는 소견이 보였다. 내원 8일째 혈관조영술을 통해서 왼쪽 A2 분절의 혈관수축을 동반한 협착과 우측 A2 분절의 혈관박리를 확인하였다. 항혈소판제제(아스피린, 클로피도그렐)와 니모디핀(90 mg/day)을 경구 투약하였고, 투약 1주일뒤 환자는 기침두통 및 벼락두통은 소실되었다. 퇴원 3개월까지 항혈소판제와 니모디핀을 사용하였고 외래에 올 때까지 증상의 재발은 없었으며, 추적 MRA에서 전대뇌동맥의 혈관연축과 혈관박리 모두 호전된 것을 확인할 수 있었다(Fig. 1).
Initial vascular imaging findings in a patient with RCVS coexisting ACA dissection. (A) CTA shows multifocal stenosis of bilateral A1 and A2 segments (arrows). (B) After 7days of CTA, MRA shows speculating dissection in right A2 segment (block arrow) and (C) sustained stenosis in left A2 segment ([B], arrow), vessel wall imaging confirms dissection in right ACA (arrow), (D), (E) Follow-up MRA and vessel wall imaging after 3months, MRA shows no vasospasm and dissection in bilateral ACA. (F) Vessel wall imaging confirms resolved dissection in right ACA. RCVS; reversible vasoconstriction syndrome, ACA; anterior cerebral artery, CTA; computed tomography angiography, MRA; magnetic resonance angiography.
질문 4. 이 환자에서 고려해야 할 사항은?
이 환자는 초기 뇌혈관영상에서 보이는 다발성 협착이 3개월이 지난 후 호전된 것을 확인하였고, 혈액검사와 뇌척수검사에서 이상소견이 발견되지 않아 RCVS로 진단하였다(Table 3). 또한 다발성 협착뿐만 아니라 전대뇌동맥에 혈관박리가 확인되었는데, RCVS와 동맥박리의 연관성은 프랑스 연구를 통해 잘 알려져 있다[3]. 그러나 서양에서는 경부혈관의 동맥박리가 두개내동맥박리보다 흔하기에 이 연구에서는 주로 경부동맥박리와 RCVS의 병발사례를 많이 보고하였는데, 국내에서는 두개내동맥박리와 RCVS의 연관성이 더 두드러지는 것으로 보인다.

일차기침두통은 기침 또는 발살바조작 등에 의해 유발되는 갑작스러운 두통이 1초에서 2시간까지 지속되며, 최소 2차례 이상 발생하는 경우 진단할 수 있다. 하지만 ICHD-3의 다른 진단으로 설명되지 않아야 한다는 점을 확인하기 위해 뇌혈관영상이 꼭 필요하다. 기침 및 발살바조작은 교감신경을 과활성시켜 혈관긴장도에 변화를 줄 수 있는 요인으로 작용한다. 교감신경의 과활성과 혈관 긴장도의 변화는 RCVS와 혈관박리의 병리 기전을 설명하는 중요한 가설이므로 기침 자체가 RCVS와 혈관박리를 발생시켰을 것이라 생각해 볼 수 있다.
본 증례의 경우 초기 CTA에서 다발성 혈관 협착이 관찰되었는데, 두통을 동반한 다발성 혈관협착의 경우 혈관연축, 혈관박리와 함께 혈관염의 가능성도 유념해야 한다. 혈관염의 경우 RCVS와 다르게 서서히 진행하는(insidious onset) 양상을 보인다. 두통은 빈번하지만, 대부분 벼락두통 양상은 아니고 일시적인 신경학적 장애와 함께 계단식(stepwise)으로 악화되는 인지저하를 동반한다. 뇌척수액검사에서 단백질 농도와 백혈구 수치 상승과 같은 염증소견을 확인할 수 있고 뇌영상에서 이상이 있는 경우가 대부분이나 보통은 비특이적이어서 진단에 주의가 필요하다. 임상적으로 RCVS와 감별하기 어렵기 때문에 조직검사를 시행할 수 있는데 침습적인 검사임에도 민감도가 낮은 경우가 있다. 따라서 최근에는 고해상도혈관벽 MRI를 이용하여 진단하는 기법이 늘어나고 있는 추세이다. 또한 류마티스인자나 항핵항체검사, 항호중구세포질항체(antineutrophil cytoplasmic antibody) 같은 면역혈청검사도 진단에 도움이 될 수 있다[4].
또한 본 증례와 달리 초기 뇌혈관 검사에서 이상소견이 발견되지 않았다면, 뇌압상승에 대한 고려를 해야 한다. 시신경유두부종을 빨리 확인하는 것이 좋으나 여의치 않다면 키아리기형이 있는지 확인 후 뇌척수액검사에서 뇌압상승의 증거를 확인하고 원인을 찾기 위해 검사를 시행해야 한다. 이 중 가장 먼저 유념해야 할 것은 뇌정맥동혈전증이다[5]. D-dimer 수치가 높고, 두개뇌압이 상승이 되어 있다면 반드시 뇌정맥동혈전증을 확인해야 하는데 이 때 MRI와 함께 magetic resonance 정맥조영(MR venography)을 시행하는 것이 좋다. 대개 서서히 시작되어 점차 심해지는 진행성의 심한 두통이고 특이양상이 없기 때문에 최근에 발생하여 지속되는 심한 두통이라면 의심해야 하고 병력청취상 혈전이 잘 유발될 만한 상황이 의심된다면 더 주의해야 한다. 기타 감별진단을 위한 진단적 알고리즘은 그림을 참고하면 된다(Fig. 2).

An algorithm for Thunderclap Headache diagnosis. HA; headache, CT; computed tomography, CTA; computed tomography angiography, MR; magnetic resonance, MRA; magnetic resonance angiography, SAH; subarachnoid hemorrhage, PACNS; primary angiitis of the central nervous system, VA; vertebral artery, CNS; central nervous system, CSF; cerebrospinal fluid, MRI; magnetic resonance imaging, LP; lumbar puncture, CA; catheter angiography, TCD; transcranial doppler. RCVS; reversible vasoconstriction syndrome. Adapted from Laura et al [4].
토 의
RCVS에서 가장 전형적인 증상은 갑자기 발생하고 호전되는 벼락두통이다. 극심한 두통이 1분 이내 최고조에 이르고, 이는 뇌동맥류 파열시 두통과 비슷하다고 한다. 보통 양측성으로 두통이 발생하고 뒤통수에서 시작하여 머리 전반적으로 통증이 퍼져나가기도 한다. 구역과 구토 빛공포증과 소리공포증이 빈번하게 동반될 수 있다. 통증이 감소되더라도 성행위, 대변보면서 배에 힘주는 행위, 스트레스나 감정적으로 불안한 상황, 운동, 기침, 재채기, 수영, 갑자기 숙였다 일어나는 행위 등에 의해 악화될 수 있다[2].
드물지만, 몇몇의 경우 신경학적 증상을 동반할 수 있다. 일시적이거나 영구적인 신경학적 결함이 8-43%정도 동반되고, 경련의 경우에도 17%까지 보고된다. 보고되는 신경학적 문제들은 대부분 시각적, 감각적, 언어 또는 운동 장애인 경우가 흔하고 일시적이라면 4시간정도까지 유지되는 경우가 있는데 편두통의 전조증상과 비슷하기 때문에 감별이 필요하다. 영구적인 손상으로 편마비, 실어증, 시야장애가 있을 수 있는데 이 경우 뇌졸중을 반드시 감별해야 한다[2].
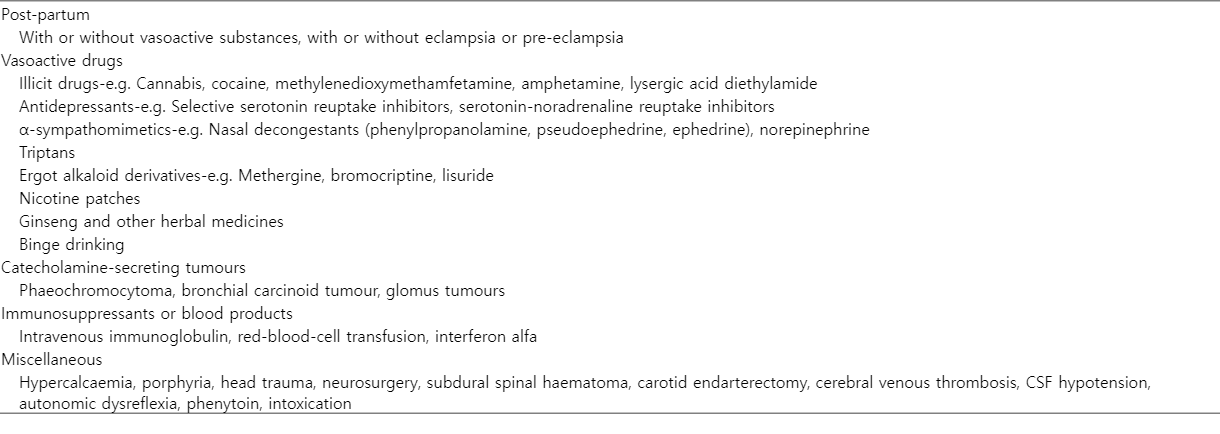
RCVS가 의심된다면 병력청취에서 기저질환과 약물복용력을 확인해야 하는데(Table 4), 대표적으로 혈관에 작용하는 약물(vasoactive drug) 과 임신기왕력을 확인해야 한다. 출산 후 1주 이내에 심한 두통과 함께 RCVS가 발견된다고 한다. 임신성 단백뇨나 Hemolysis, Elevated Liver enzymes, and Low Platelet count 같은 질환이 임신중 없었더라도 정상적인 출산 이후에도 RCVS가 발생할 수 있으므로 최근 출산한 병력이 있는 젊은 여성의 경우 극심한 두통이 갑자기 발생했다면 RCVS 가능성을 유념해야 한다. 또한 RCVS 같은 경우에 비파열성뇌동맥류나 경동맥 또는 척추동맥의 혈관 박리가 병발되어 있는 경우가 있다. RCVS의 핵심적인 병태생리기전은 혈관긴장도의 변화로 인한 혈관의 수축인데, 아직 RCVS와 혈관박리 중 어떤 것이 선행 질환인지는 밝혀지지 않았다[2].
RCVS 치료에 무작위 배정으로 진행한 임상연구는 없지만, 질환을 빨리 인지하여 치료를 하는 것이 예후 개선에 도움이 된다. 두통을 악화시킬 수 있는 모든 행위는 중단하고, 복용하고 있는 약물 중에 악화시킬 수 있는 약물이 있다면 중단하며 최대한 편하게 쉴 수 있는 환경을 제공해야 한다. 동시에 혈관 연축에 대한 치료를 진행하게 된다. 보통 니모디핀 같은 칼슘통로차단제(매 4-8시간마다 30-9 0mg)을 4-12주 사용하며 일반적으로 투약 후 48시간이내에 벼락두통은 감소한다. 이외에도 베라파밀이나 황산 마그네슘을 사용하기도 한다. 경구 니모디핀 투약에도 불구하고 두통이 심하거나 혈관수축이 심하거나 허혈성 합병증이 동반된 경우에는 몇몇 보고에서 혈관 내 주사제로 니모디핀을 주사하는 경우가 있다. 스테로이드는 증상을 악화시킨다는 보고가 있어 투약을 지양하는 것이 좋다[2,3].
KEY POINTS
1. 벼락두통과 뇌 영상검사
• 벼락두통은 보통 1분 이내에 통증이 최고조에 이르고 이제까지 경험하지 못한 강도의 심한 두통을 말한다. 주로 갑자기 깨질 듯이, 망치로 내려치듯이 아프다고 말하기도 하며 생명을 위협할 수 있거나 장애를 일으키는 이차두통의 발현증상으로 나타나므로 감별진단이 중요하다.
• 여러 뇌혈관질환이나 두개내 이상이 벼락두통의 원인이 될 수 있다. 특히 거미막하출혈, RCVS, 뇌동맥박리, 뇌정맥혈전증은 드물지 않게 발현되기 때문에 중요한 감별진단이다. 이를 위해 뇌영상 검사를 시행하는 것이 권고된다. CT나 MRI/MRA를 통하여 벼락두통이 발생할 수 있는 원인을 감별할 수 있다.
2. RCVS
• 벼락두통과 함께 뇌혈관검사에서 다발적인 불규칙한 혈관 협착이 발견되었다면 의심해볼 수 있고, 12주 이내에 뇌혈관이 일부 또는 모두 호전된 경우 진단할 수 있다.
• 혈관에 작용하는 약물 복용력이나 기저 질환이 선행되어 있을 가능성이 높아 병력청취가 중요하다. 두통이 악화되는 유발 요인을 파악하여 피하도록 하여야 한다.
• 벼락두통과 함께 뇌혈관 검사에서 이상이 발견되는 다른 질환들과의 감별이 필요하다.
• 치료는 칼슘 통로차단제인 니모디핀이 주로 사용되며 4-12주정도 복용이 권고된다.