약물난치성 뇌전증 환자의 약물 치료 권고사항: 2021 대한신경과학회 진료지침 뇌전증 분과 소위원회
Practical Drug Treatment Recommendations on the Drug Refractory Epilepsy Patients: 2021 Clinical Guideline Subcommittee for Epilepsy in the Korean Neurological Association
Article information
Trans Abstract
One third of the overall epilepsy population are estimated to be a drug refractory epilepsy (DRE), defined as the patients who failed to control seizure reduction, even tried two or more appropriate antiepileptic drugs (AEDs) trials. Those people need additional AEDs trials or other treatment options (resective surgery, neuromoulation, etc.). Here, we, clinical guideline committee of the Korean Neurological Association (KNA) introduce the recommendations of AEDs treatments including not only old and new AEDs currently available in Korea but also AEDs planned to be launched in the new future for DRE patients with literature review to help efficient decision of the clinician. The authors reviewed literatures and assessed efficacy and tolerability on 12 currently available and four newly introduced/or planned AEDs applied to DRE patients, published from November 2015 to July 2021. Brivaracetam, eslicarbazepine, canabidiol and cenobamate are the four AEDs that are newly introduced or planned to be launched soon. The reviewed articles are publications after November 2015, 2018 American Association of Neurology guideline, new AEDs which were introduced or planned to be launched as of 2021. All AEDs are classified based on the therapeutic rating scheme, generating recommendations. Overall 173 papers have been reviewed and analyzed for recommendation rationales. KNA introduce additional add-on treatment or conversional monotherapy guidelines on the drug refractory focal and generalized epilepsy. We hope these guidelines or recommendations to help clinical decision for the treatment of drug refractory epilepsy patients
서 론
뇌전증은 뇌졸중, 치매와 더불어 3대 주요 뇌신경질환으로 분류되고, 국내 환자는 약 35만 명으로 추산되는 비교적 흔한 중추신경계질환이다[1]. 진단 후 1차 치료로서 뇌전증약(antiepileptic drugs [AEDs] 혹은 antiseizure medication)을 이용한 약물 치료가 원칙이며, 60-70%의 환자가 한 가지 혹은 두 가지 뇌전증약 치료를 통해 증상이 호전되거나 완전히 조절된다. 그러나 뇌전증 환자의 약 30%는 적절한 뇌전증약을 두 가지 이상 충분한 용량으로 복용하였음에도 불구하고 발작 조절이 안 되는 약물난치성 뇌전증으로 진행하며, 이들은 심리사회적 문제, 동반질환의 증가 등 여러 가지 어려움을 겪게 된다[2,3].
일반적으로 뇌전증은 만성 질환으로 분류되고 있으며, 약물난치성 뇌전증의 경우 건강의료보험급여에서 산정특례 적용 대상이 되는 중증 난치성 질환이다.
해외 사례를 살펴보면, 미국신경과학회(American Association of Neurology, AAN)는 새롭게 진단받은 뇌전증과 약물난치성을 구분하여 진료지침을 권고하고 있으며, 영국 국립보건임상연구소(National Institute for Health and Clinical Excellence)에서도 난치성 뇌전증(refractory epilepsy)에 대한 치료지침을 구분하고 있다.
뇌전증 치료제에 관한 문서화된 기존 국내 지침은 2015년에 대한뇌전증학회에서 편찬한 뇌전증의 약물 치료지침[4]이 있으며, 임상 의사들이 뇌전증 환자를 진료함에 있어 참고할 수 있는 자료로 활용되어 왔다. 하지만 2015년 이후로 약물난치성 뇌전증 환자에게 사용할 수 있는 새로운 약물들이 국내에 속속 도입되었고, 2018년에는 미국신경과학회(AAN)에서 약물난치성 뇌전증 환자를 위 한 뇌전증약 진료지침[5]을 발표한 바 있다. 이에 대한신경과학회는 현재 국내외에서 사용 중인 약물난치성 뇌전증에서의 뇌전증약에 관한 체계적인 검토와 고찰을 근거로 하여 현실에 적합한 새로운 지침 혹은 권고사항을 마련함으로써 임상 의사들이 약물난치성 뇌전증 환자를 치료함에 있어 임상적 판단에 도움을 주고자 하였다.
방 법
국내 가이드라인이 2015년 출간된 점과 미국신경과학회의 약물 난치성 뇌전증 치료지침이 2015년까지의 문헌을 검토한 점을 고려하여, 본 조사에서 검토할 문헌은 2015년 11월부터 2021년 7월 1일까지 기간 동안 PubMed에 색인된 영문 논문으로 정하였다.
적용된 총 16종의 약물은 clobazam, vigabatrin, zonisamide, lamotrigine, gabapentin, tompiramate, oxcarbazepine, levetiracetam, pregabalin, lacosamide, rufinamide, perampanel, brivaracetam, eslicarbazepine, canabidiol, cenobamate였다. 이들 약물에 관한 논문 가운데 제목(title), 초록, 환자군 외에 약물 치료 실패군(drug treatment failure), 치료저항(treatment resistant), 불응(refractory), 난치(intractable), 약물저항(pharmacoresistant), 조절되지 않는(uncontrolled)과 같은 용어가 포함된 임상 문헌을 중심으로 검토하였다.
선정기준, 제외기준 및 근거 분류기준은 미국신경과학회의 2004년 약물난치성 뇌전증 환자 진료지침 선정기준을 토대로 분류하였다. 선정기준으로는 뇌전증 환자 대상으로 1) 효능, 안전성, 내약성, 작용기전 연관 임상, 2) 사람 대상, 3) 무작위 배정, 코호트, 사례분석, 관찰 연구, 증례 시리즈, 4) 영문으로 게재된 논문을 포함하였다. 반면, 1) 논문의 제목 혹은 초록 및 방법에서 약물난치성 뇌전증을 의미하는 단어가 포함되지 않은 경우, 2) 뇌전증 환자가 아닌 경우, 3) 16종에 포함된 약물 사용이 아닌 경우, 4) 결과 지표가 없는 경우, 5) 기간에 해당하지 않는 경우, 6) 초록만 발표된 경우는 배제하였다.
근거 분류기준에서 Class I에는 전향적, 무작위 통제시험이 이루어졌으며, 환자군을 대표할 수 있는 환경에서의 결과 평가를 제시한 논문이 포함되었다. 또한 1) 주요 결과, 2) 포함/배제기준, 3) 편향(bias)의 가능성을 낮출 drop-out 및 cross-over의 제시, 4) base-line 특징의 제시 및 치료 환자군이 baseline 특징과 동일할 것이며, 이를 뒷받침할 수 있는 통계적 조정의 조건들이 만족되어야 한다. Class II의 경우 대표 환자군에서의 전향적 코호트 연구를 가림(masking)된 결과 평가 포함 및 Class I의 1)-4)를 만족하거나 1)-4) 중 하나를 제외한 모든 조건 만족 및 대표 환자군에서의 무작위 대조군 연구(randomized clinical trials)를 실행한 논문이 해당된다. Class III은 Class I 및 II 안에 포함되지 않는 통제시험이 포함되며 결과 평가가 환자 치료의 독립적인 시험일 경우에 분류된다. Class IV는 통제되지 않은 연구에서의 증거, 증례보고 및 전문가 보고서가 해당된다. 권고사항은 근거분류기준[5]에 따라 A-D로 분류하였고, Class IV에 해당되는 문헌은 배제하고 분석하였다(Table 1).

Criteria for inclusion & exclusion of article search and evidence classification (based on 2004 AAN criteria for article review)
결 과
2015년 11월부터 2021년 7월까지 연구 대상인 16종의 2, 3세대 뇌전증약 가운데 선정기준을 만족하는 문헌 중에서, Class IV 기준 문헌은 배제하고 총 173건의 논문을 본 진료지침 작성에 반영하였다. 권고사항에는 만약 새로운 업데이트가 없거나, 확인된 문헌이 Class IV에 해당하는 경우, 업데이트 이전의 문헌을 검토하여 권고사항과 함께 나열하였다(Table 2).
Summary of recommendations of 12 currently available and 4 newly introduced/or planned AEDs applied to drug refractory epilepsy patients focused on level A and level B evidence
1. 성인 난치성 국소 뇌전증에서의 부가요법
1) 2015년 현재 우리나라에서 처방 중인 뇌전증약
성인 난치성 국소 뇌전증의 부가요법에는 gabapentin, lamotrigine, oxcarbazepine (extended release 제형 포함), zonisamide가 효과적으로 확인되었다[5]. 이후 levetiracetam, clobazam, eslicarbazepine, lacosamide, perampanel, pregabalin, rufinamide, vigabatrin, topiramate-ER, cenobamate, brivaracetam에서 난치성 환자군에 대한 추가적 연구를 수행하였다.
(1) Clobazam
Clobazam은 1981년 도입되었고, 뇌전증약 단독요법으로 충분히 조절되지 않는 뇌전증 환자에 있어서 보조 치료로 식약처의 승인을 받았다. Clobazam은 진정 효과가 적은 뇌전증약으로 개발되었으며, GABAA 수용체의 5개 소단위 중 알파/감마 소단위에 결합하고 염소이온통로 개폐 빈도 증가로 GABA 매개 신경세포 억제를 촉진한다[6,7].
Clobazam은 3편의 Class III 임상을 통해 평가되었다. 새로 추가된 임상은 없었으며, 현재까지 약물난치성 국소 뇌전증 환자 대상 출판된 임상은 3편의 Class III 연구로[8-10] 발작 빈도의 유의한 감소와 높은 반응률을 보였다. 그러나 소수의 참가자 대상이며, 하나의 논문에서는 전신성 뇌전증까지 포함되어 있다. 주된 부작용으로는 진정, 어지럼, 신경과민, 우울, 탈억제가 있었다.
Recommendation
Clobazam에 관해 새로운 추가 연구는 없었다. 기존의 기준에 따라, 치료 저항성 성인 국소 뇌전증에 대한 추가 병용요법에 효과적이다. (3편의 Class III, Level C; Week)
(2) Vigabatrin
1994년 다른 뇌전증약으로 충분히 조절되지 않거나 다른 뇌전증약과 병용요법을 실시할 수 없는 약물난치성 부분 뇌전증(2차성 전신화 발작의 유무에 관계없이) 환자에 대하여 다른 뇌전증약과의 병용요법 및 영아연축(West syndrome)의 치료에 대한 단독요법으로 식약처의 허가를 받았다. GABA aminotransferase를 비가역적으로 억제하여 GABA 농도를 올려 결과적으로 GABA의 활성을 증가시켜 항경련 작용을 하는 기전이다[6,7].
Vigabatrin은 2편의 Class I 연구를 검토하였다. 새로 추가된 vigabatrin의 성인 난치성 국소 뇌전증에 대한 효과 임상은 없었으며, 현재까지 약물난치성 국소 뇌전증 환자 대상 출판된 임상은 2편의 Class I 연구로[11,12] 위약 대비 유의한 높은 반응률 및 매달 발작 빈도의 중앙값 감소를 보였다.
부작용으로는 진정, 피곤함, 어지럼 등이 있다. Vigabatrin의 축적 용량이 비가역적 망막병증으로 인한 양측 시야 수축[13] 및 비가역적 양측성 시야 협착이 유발될 수 있어 약물 투약시 주의가 필요하다[6,7]. 따라서, 정기적인(미국 Food and Drug Administration [FDA]에서는 3개월마다) 시야검사를 권고한다. 꾸준히 vigabatrin과 망막 구조 및 기능에 대한 논문이 출판되고 있다.
Recommendation
Vigabatrin에 관한 새로운 추가 연구는 없으며, 기존의 기준에 따라, 약물난치성 국소 뇌전증에 대한 추가 병용요법에 효과적이다. (2편의 Class I, Level A; Strong)
(3) 서방형 topiramate (TPM-ER)
2017년 새로 뇌전증으로 진단된 2차성 전신발작을 동반하거나 동반하지 않는 부분발작의 치료(4세 이상)의 단독요법, 그리고 1) 기존 1차 뇌전증 치료제 투여로 적절하게 조절이 되지 않는 2차성 전신발작을 동반하거나 동반하지 않는 부분발작의 치료(4세 이상), 2) 청소년 간대성 근경련 뇌전증(juvenile myoclonic epilepsy, JME) 환자의 근간대성 발작의 치료(12세 이상), 3) 특발성 전신성 뇌전증(idiopathic generalized epilepsy) 환자의 1차성 전신 강직간대 발작의 치료(12세 이상)의 부가요법으로 승인을 받았다.
다양한 작용기전을 가지고 있으며, AMPA 수용체의 대항제로 작용, 전압-의존성 나트륨 이온통로 차단, GABAA 수용체의 소단위와 상호작용하여 GABA-유래 염소 이온전류를 향상시켜 항뇌전증효과를 나타낸다[6,7].
Topiramate-ER은 한편의 Class 1 임상으로 조사되었으며, 확인된 topiramate (ER) (200 mg/day)의 위약 대비, 50% 반응률 및 주간 발작 감소 중앙값이 우월하였다. 가장 빈번한 부작용으로는 졸음, 이상감각, 체중 감소가 있었다.
Recommendation
Topiramate-ER은 난치성 뇌전증 환자에게 부가요법으로 효과적이다. (1편의 Class I, Level B; Moderate)
(4) Levetiracetam
2002년 새로 뇌전증으로 진단된 이차성 전신발작을 동반하거나 동반하지 않는 부분발작(4세 이상)의 단독요법 및 1) 기존 1차 뇌전증 치료제 투여로 적절하게 조절이 되지 않는 이차성 전신발작을 동반하거나 동반하지 않는 부분발작의 치료(4세 이상), 2) 청소년 간대성 근경련 뇌전증(JME) 환자의 근간대성 발작의 치료(12세 이상), 3) 특발성 전신성 뇌전증(idiopathic generalized epilepsy) 환자의 1차성 전신 강직-간대 발작의 치료(12세 이상)의 부가요법으로 식약처의 승인을 받았다.
시냅스 전 신경세포의 synaptic vesicle glycoprotein 2A (SV2A) 단백 결합으로 SV2A 단백과 결합하면 시냅스 소포의 모양 변형으로 신경전달물질 소포내 저장이 영향을 받아 exocytosis가 이루어지지 못한다. 이 기전을 통해 신경전달물질 분비를 조절하여 항뇌전증효과를 보인다.
Levetiracetam은 한편의 Class III 연구에서 평가되었으며, 브라질에서 성인 및 약 45% 이상 소아가 포함되었고, 50% 반응률에서 levetiracetam군(1,000-3,000 mg/day)에서 위약군 대비 큰 달성을 보였고, 주당 발작 횟수에 따른 50% 발생률이 위약군 대비 유의하게 높았다. 위약군과 유사한 안전성이었고, 상위 3개의 부작용은 신경계, 감염, 위장관계 문제였다[14].
Recommendation
Levetiracetam은 치료 저항성 성인 국소 뇌전증에 대한 추가 병용요법으로 사용을 고려할 수 있다. (1편 Class II, Level C; Weak)
(5) Pregabalin
2005년 성인에서 이차적 전신발작을 동반하거나 동반하지 않은 부분발작의 보조제(부가요법)로 허가를 받았다. 신경세포의 시냅스 전 전위의존성칼슘통로의 알파2델타 소단위에 결합해 칼슘유입을 억제하여 흥분성 신경전달물질(글루타메이트, 노르아드레날린, substance P 등)의 방출을 억제한다. 구조적으로 GABA유사체로 알려져 있지만, GABA수용체와 관련은 없다[6,7]. Pregabalin은 속효성(immediate releasr, IR) pregabalin (PGB-IR)에 관한 Class I 연구 2편과 Class II 연구 3편[15-19] 그리고 방출제어(controlled release, CR) pregabalin (PGB-CR)에 관한 Class I 연구 1편[20]이 평가되었다.
Pregabalin 150, 300, 600 mg/day 투약은 위약 대비 유의하게 우월하였으며, >50%의 반응률을 보였고 용량의존적인 방식으로 발작 감소율 중앙값이 위약에 비해 높았다. 어지럼 및 진정은 가장 빈번하게 발생한 부작용이었다. 부작용 관련 투약 중단도 보고되었고, 그 빈도는 용량에 비례하여 증가하였다.
한 Class I 연구에서 위약과 속효성 PGB 165 및 330 mg/day를 비교하였다[15]. 세 군 간의 차이는 확인되지 않았다. 부작용과 부작용 관련 투약 중단은 고용량군에서 높게 나타났으며 속효성 PGB에 관한 다른 임상시험과 비슷하게 나타났다[16-18].
새로 확인된 한편의 Class II 임상에서 gabapentin에 비해 baseline부터 변화율 평균 및 중앙값에서 열등하지 않음을 확인하였다. 가장 빈번한 부작용으로는 양 군에서 졸림, 어지럼, 체중 증가, 두통, 입마름이었다[19].
Recommendation
성인 약물난치성 국소 뇌전증에서 속효성 PGB의 추가(add-on) 병용요법은 효과적이다. (2편의 Class I, 3편의 Class II, Level A; Strong) 유효성과 부작용은 용량에 비례하여 증가하였다. PGB-CR은 유효성을 결정하기에는 근거가 부족하다. (1편의 Class I, Level B; Moderate)
(6) Lacosamide
2016년 16세 이상의 뇌전증 환자에서 2차성 전신발작을 동반하거나 동반하지 않는 부분발작 치료의 부가요법으로 식약처의 허가를 받았다. 전압의존성 나트륨 이온통로에 작용하여 선택적으로 저속 비활성화를 촉진시켜 신경세포의 흥분성을 억제한다[6,7].
Lacosamide는 Class I 연구 3편과 Class II 연구 2편에서 lacosamide와 위약을 비교하였다[21-24]. Lacosamide 400 및 600 mg/day 투약은 위약 대비 유의하게 높은 반응률과 발작 감소율 중앙값을 보였다. 한 Class II 연구[22]에서 2차성 전신 강직간대성 발작 감소에 대해 600 mg/day가 더 큰 효과를 보였다. 부작용(adverse reaction)으로 인한 약물 중단은 없었다. Class I 연구에서 보고된 부 작용은 복시, 현기증, 구토였고[21] Class II 연구에서는 어지럼, 오심, 피로감, 운동실조, 복시, 안진이 있었다[22,23]. 한 Class III 연구에서는 lacosamide 비경구 제형을 평가하였다[24]. 두통, 어지럼, 졸음이 가장 흔한 부작용이었으며, 400 mg/day 이상 용량에서 빈도가 증가하였다.
새로 확인된 Class I 연구 한 편은 중국인 및 일본인 대상으로[25] lacosamide군(200 mg/day 및 400 mg/day)과 위약군으로 구성되었고, 위약군 대비 발작 횟수가 감소하였다. Lacosamide 200, 400 mg/day군에서 위약 대비 유지 기간에서 28일 주기-발작 횟수 감소율이 유의하였고, 다른 글로벌 임상과 일관되게 중국 및 일본인에게도 lacosamide 200, 400 mg/day는 효과적으로 확인되었다. 10% 이상 빈번히 발생되는 부작용은 위약군 대비 lacosamide군에서 어지럼과 졸음이었으며, lacosamide 연관 가장 빈번한 부작용은 신경계, 위장 관계 문제였고 용량의존적이었다. 위약군 대비 더 높은 부작용 사례는 기존 임상에서 언급된 내용과 유사하다.
Recommendation
Lacosamide는 확실히 약물난치성 국소 뇌전증에 효과적이다. (3편의 Class I, 2편의 Class II, Level A; Strong)
(7) Rufinamide
2009년 1세 이상의 환자에서 레녹스-가스토증후군과 관련된 발작 치료 시 부가요법으로 식약처의 허가를 받았다. 나트륨 이동통로를 차단하여 항뇌전증 작용을 한다[6,7].
Rufinamide는 3편의 Class I 연구에서 rufinamide와 위약을 비교하였다[26-28]. Rufinamide는 28일간의 발작 빈도 중앙값 감소 및 50%의 반응률에서 위약 대비 우월하였으며, 최저 유효 용량은 400 mg/day였다. 일관되게 적절한 효과를 보였다. 가장 빈번한 부작용으로 어지럼, 피로감, 오심, 졸음, 복시, 혼동, 운동 실조, 집중력저하가 있었다.
Recommendation
Rufinamide는 레녹스-가스토증후군에 대한 추가 병용요법으로 효과가 있으나, 치료 유익성은 미미하다. (3편의 Class I, Level A; Strong)
(8) Perampanel
2015년 국소 뇌전증 환자의 이차성 전신발작을 동반하거나 동반하지 않는 부분발작의 치료(만 4세 이상)의 단독요법 및 1) 뇌전증 환자의 이차성 전신발작을 동반하거나 동반하지 않는 부분발작의 치료(만 4세 이상), 2) 일차성 전신 강직간대 발작: 특발성 전신 뇌전증(idiopathic generalized epilepsy) 환자의 일차성 전신 강직간대 발작의 치료(만 7세 이상)의 부가요법에 식약처의 허가를 받았다.
Non-NMDA수용체의 하나인 AMPA에 선택적 대항제로 작용하며, 흥분성 신경흥분전달계인 글루타민산에 작용하는 이온친화성 글루타민수용체(inotropic glutamate receptor) 가운데 AMPA수용체는 글루타민성 흥분의 시작과 동기화를 일으키면서 발작을 유도하는 데 중요한 역할을 한다[6,7].
Perampanel은 4편의 Class I, 1편의 Class III 연구에서 perampanel과 위약을 비교하였다[29-33]. Perampanel 4, 8, 12 mg/day 용량은 28일간 발작 감소율 중앙값에 대해 위약 대비 우월한 소견을 보였다. 매우 높은 위약 비율로 인해 perampanel의 용량 반응 비율은 연구별로 차이를 보였다. 가장 흔한 부작용은 어지럼, 운동 실조, 낙상, 두통, 졸음, 피로감, 신경과민, 우울, 오심, 체중 증가이다. 부작용은 용량의존적이며 적정(titration) 기간과 유지 기간에서 모두 발생하였다. 신경과민과 공격적인 행동으로 인해 제품 설명서에 경고문이 들어가게 되었다.
새로 확인된 임상은 Class I, Class III 각각 한 편이었다[32,33]. Class I인 아시아태평양지역 연구는 perampanel 8, 12 mg/day군에서 위약 대비 28일간 발작 감소율 중앙값에 유의한 결과를 보였다[32]. Class III 한 편의 연구(post-hoc)에서 perampanel 4 mg/day군이 위약 대비 28일간 발작 감소 중앙값이 부분발작뿐만 아니라 전신 강직간대 발작도 유의하게 감소되었고, enzyme-inducing AEDs보다 그렇지 않은 AEDs에서 더 좋은 발작 개선을 보였다[33]. 두 임상을 종합하여 perampanel의 부작용에는 어지럼, 졸음, 비인두염, 상기도감염, 두통, 예민해짐, 구역, 피로, 보행이상, 피부발진이 있었다.
Recommendation
Perampanel은 약물난치성 성인 국소 뇌전증에 대한 추가 병용요법으로 효과가 있는 것이 확인되었다. (4편 Class I, 1편 Class III, Level A; Strong)
2) AEDs newly approved by Korean FDA after 2016 or AEDs planned to be launched in the new future for DRE patients (Table 3)

AEDs newly approved by Korean FDA after 2016 or AEDs planned to be launched in the new future for DRE patients
(1) Cenobamate
Cenobamate는 가까운 미래에 국내 도입 예정인 뇌전증약으로 현재 2021년 기준 국내 미허가 상태이며, 아시아인(한국, 일본, 중국) 대상 3상시험을 진행 중이다. 미국 식약처(FDA)에 의해 성인 부분(국소)발작 치료제로 승인을 받았다. 기존의 나트륨 이온통로 차단제와 다른 결합부위로 나트륨 이온통로를 차단하는 것으로 알려졌고, GABAergic transmission 또한 강화하는 것으로 확인되었다[6,7].
성인 약물난치성 국소 뇌전증에 대한 cenobamate의 결과는 두 편의 Class I, 한 편의 Class III 연구가 평가되었다[34-36]. 한 개의 Class I 연구가 cenobamate 200 mg/day와 위약군 비교였고 6주간의 유지 기간을 확인한 2상 임상이었다[34]. 28일간 발작 감소 중앙값 및 50% 반응률 모두 위약 대비 유의하게 확인되었다.
다른 Class I 임상에서 cenobamate 100, 200, 400 mg/day와 위약군을 비교하였고 12주의 유지 기간을 둔 2상 임상이었다[35]. 위약군 대비 cenobamate 100, 200 400 mg/day 임상에서 200, 400 mg/day에서 28일간 발작 감소 중앙값이 유지 기간에서 유의하게 높았다. 50% 반응률은 모든 용량에서 위약 대비 유의한 결과를 보였다.
하나의 Class III 임상에서는 2상에서 확인된 악물 부작용(drug reaction with eosinophilia and systemic symptoms, DRESS)의 안전성 이슈로 3상 임상으로 진행되어, cenobamate 25-400 mg/day에서의 DRESS 발생과 장기 안전성을 확인하였고, DRESS는 확인되지 않았지만 약물 투여 시 천천히 적정하기를 권유한다[36]. 공통된 가장 흔한 부작용은 졸음, 어지럼, 두통, 피로였고, Class I 하나의 임상에서 복시가 추가로 보고되었다.
Recommendation
Cenobamate는 성인 약물난치성 국소 뇌전증에 대한 추가 병용 요법으로 효과적임이 확인되었다. (4편 Class I, 1편 Class III, Level A; Strong)
(2) Eslicarbazepine
Eslicarbazepine은 새로 뇌전증으로 진단된 성인에서 이차성 전신발작을 동반하거나 동반하지 않은 부분발작 치료의 단독요법과 만 6세 이상의 소아 및 성인에서 2차성 전신발작을 동반하거나 동반하지 않은 부분발작 치료의 부가요법으로 허가를 받았다. 전압 의존성 나트륨채널 억제제로 밝혀졌으며, 추가로 T형 칼슘채널에서 항경련 효과를 보인다[6,7].
Eslicarbazepine은 5편의 연구(2편의 Class I, 1편의 Class II, 2편의 Class III 연구)에서 eslicarbazepine과 위약을 비교하였다[37-41]. 각 Class I, II, III 연구에서 400, 800, 1,200 mg을 하루 1회 투여하는 조사를 하였다. 3편의 연구에서 800 및 1,200 mg/day 용량으로 4주간의 발작 빈도가 유의하게 감소하였고[37-39] Class I 및 Class III 연구에서는 반응률이 유의하게 높은 소견을 보였다. Class I 연구에서 무발작 비율은 1,200 mg 용량에서 더 높았다. 투약 중단을 초래한 부작용을 포함하여, 치료관련 부작용은 일반적으로 용량의존적인 경향을 보였다. 가장 빈번한 부작용은 어지럼, 두통, 복시, 졸음, 오심, 구토, 조정장애가 있었다.
각각 한 편의 Class I 및 Class III 임상이 확인되었으며[40,41], Class I 임상은 위약 대비 eslicarbazepiner군(1,200 mg/day)에서 치료 후 평균 발작중증도설문지(seizure severity questionnaire, SSQ)의 총점수가 유의하게 감소함을 확인하였다. 또한, 평균 SSQ, 총점수 발작 동안 의식 변화(altered consciousness during seizures, DS), 발작 후 신체 회복(physical aspects of postictal recovery after seizures)과 전반적 중증도와 불편함(overall severity and bothersomeness, SB)은 eslicarbazepine 800 mg/day에서 위약군 대비 유의하게 감소되었다. Eslicarbazepine 두 군(800, 1,200 mg/day)에서 위약군 대비 평균 TS, DS, SB는 유의하게 차이를 보였다[40]. 다른 Class III 임상은 4개의 3상 임상을 통합해 분석하였고, eslicarbazepine 400, 800, 1,200 mg이 평가되었으며 위약군 대비 발작 감소는 800, 1,200 mg에서 위약군 대비 유의하였다[41]. 가장 흔한 부작용으로는 졸음, 어지럼, 구역이 보고되었다. 부작용은 용량 의존적이었다.
Recommendation
Eslicarbazepine 800 및 1,200 mg/day 용량은 확실히 약물난치성 성인 국소 뇌전증의 치료에 효과적이다. (2편의 Class I, 1편의 Class II, 2편의 Class III, Level A; Strong)
(3) Brivaracetam
2019년 16세 이상의 뇌전증 환자에서 2차성 전신발작을 동반하거나 동반하지 않는 부분발작 치료의 부가요법에 식약처의 승인을 받았다.
Levetiracetam와 유사하게 SV2A에 작용하여 신경전달물질의 exocytosis를 방해하여 항뇌전증 역할을 하며, levetiracetam보다 15-30배 더 높은 친화력을 보이고, 빠른 작용(rapid onset)을 하는 뇌전증약이다[6,7].
Brivaracetam은 네 편의 Class I 연구로 평가되었으며, 위약군 대비 brivaracetam의 효능을 확인하였다. 한 편[42]은 brivaracetam 5, 20, 50 mg/day, 다른 한 편[43]은 brivaracetam 20, 50, 100 mg/day에서, 나머지 한 편[44]은 levetiracetam 노출자를 제외하여 brivaracetam 100, 200 mg/day에서 진행되었다. 각 임상의 용량별 결과가 상이한 것을 보완하여 pooled-analysis가 진행되었고, brivaracetam의 50, 100, 200 mg/day와 위약군을 비교하였다. 28일 기점 발작 횟수 감소 및 50% 반응률은 위약 대비 모든 용량군에서 유의하게 개선되었다. 무발작률(seizure free rate)에서는 100, 500 mg/day군에서 위약 대비 유의한 결과를 보였다[45]. 가장 빈번하게 나타난 부작용은 졸음, 어지럼, 두통, 피로였다.
Recommendation
Brivaracetam는 성인 약물난치성 국소 뇌전증 환자에게 부가요법으로 효과적이다. (4편의 Class I, Level A; Strong)
3) 5가지 이상 뇌전증약에 실패한 경우 새롭게 시작하는 부가요법
한 편의 Class II 연구에서 brivaracetam과 위약 대비, 이전에 5개 이상의 뇌전증약에 실패한 환자군을 대상으로 사후분석이 진행되었고, 50, 100, 200 mg/day의 brivaracetam은 위약 대비 28일 간 발작 빈도가 유의하게 줄었으며, 각 연구에서 용량별 치료 반응률이 상대적으로 높은 것으로 확인되었다. 무발작률은 100 mg/day 군에서 5.8%로 위약군의 0%보다 유의하게 높았다[46]. 현재까지 5개 이상의 뇌전증약이 실패한 환자에게서 뇌전증약의 효능을 입증한 임상으로 본 임상이 유일하다.
Recommendation
5개 이상의 뇌전증약에 실패한 약물난치성 성인 국소 뇌전증 환자에게 부가요법으로 효과적일 수 있다. (1편의 Class II, Level C; Weak)
4) 성인 약물난치성 국소 뇌전증 환자에서의 약물 치료: 결론
성인 약물난치성 국소 뇌전증 환자에서 Level A; Strong 약물은 vigabatrin, pregabaline, lacosamide, rufinamide, perampanel, cenobamate, eslicarbazepine, brivaracetam으로 부가요법에 효과적이다.
Topiramate-ER, pregabalin-ER은 Level B; Moderate로 부가요법에 효과적일 수 있다. Levetiracetam, clobazam은 Level C; Weak로 부가요법에 아마도 효과적일 수 있다.
새로 승인되었거나 곧 도입 예정인 약물은 cenobamate, eslicarbazepine, canabidiol, brivaracetam이 있으며, brivaracetam은 성인의 과거 5개 이상의 약물로 발작 조절에 실패한 환자에게 임상 근거(Level C; Weak)가 있으며, 다수의 뇌전증약에 실패한 환자에게 임상적 옵션이 될 수 있다.
2. 성인 난치성 국소 뇌전증에서의 단독요법
현재까지 약물난치성 성인 국소 뇌전증에 대해 lamotrigine, oxcarbazepine 및 topiramate가 효과적이라고 알려져 있고, 5편의 Class III 단독요법으로 전환 투여를 실시한 연구가 수행되었다. 새로 확인된 연구는 없었으며, 기존의 1편의 연구[47]에서 extendedrelease levetiracetam (LEV-XR)을, 1편의 연구[48]에서 pregabalin을, 1편의 연구[49]에서 lacosamide를 그리고 나머지 2편의 연구[50,51]에서 eslicarbazepine을 평가하였다.
LEV-XR 연구[47]에서는 1,000, 2,000 mg/day의 용량이 사용되었고, pregabalin 연구[48]에서는 150, 600 mg/day 용량이 사용되었다. Lacosamide의 경우 300, 400 mg/day 용량과 과거 대조군을 비교하였다[49]. Eslicarbazepine 연구에서는 1,200 및 1,600 mg/day의 용량을 조사하였다[50,51].
상기 4가지 약물 모두에서 예상 종료율이 높은 용량의 LEV-XR 및 pregabalin에 무작위 배정된 환자에서 유의하게 낮게 나타났으며 lacosamide와 eslicarbazepine은 두 가지 용량에서 모두 탈락률이 대조군에 비해 높았다. LEV-XR에 의해 가장 빈번하게 발생한 부작용은 졸음, 두통, 경련이 있었으며 두 용량 간 차이는 없었다. Pregabalin의 경우, 가장 빈번한 부작용은 이전에 설명한 pregabalin 추가 병용요법에 관한 연구에서 보고된 바와 유사하였다[17,18,20].
Lacosamide의 경우 가장 흔한 부작용은 어지럼, 두통, 오심, 경련, 졸음, 피로감이 있었으나 400 mg 투약군에서 졸음이 더 많이 발생한 것을 제외하면 두 용량 간 차이가 없었고 대부분이 경도 내지 중등도 증상이었다. Eslicarbazepine의 경우 가장 빈번한 부작용은 어지럼, 두통, 피로감, 졸음, 오심, 비인두염이었으며, 용량 의존적으로 발생하였다.
Recommendation
Eslicarbazepine은 단독요법으로 약물난치성 성인 국소 뇌전증에 효과적일 수 있다. (2편의 Class III) 약물난치성 성인 국소 뇌전증에 단독요법으로서 lacosamide, LEV-XR 또는 pregabalin의 유효성을 결정하기에는 근거가 부족하다. (각 약제별로 1편씩의 Class III 연구)
1) 성인 난치성 국소 뇌전증에서의 단독요법: 결론
성인 난치성 국소 뇌전증에서 발작 빈도를 줄이기 위해 eslicarbazepine 단독요법이 고려될 수 있다(Level C). 다른 2세대 또는 다른 3세대 뇌전증약을 단독요법으로 권고하기에는 아직 근거가 부족하다(Level U).
3. 성인 및 소아 난치성 전신 뇌전증에서의 부가요법
1) 난치성 전신 강직간대성 발작을 동반한 전신 뇌전증
기존의 약물난치성 전신 강직간대성 발작을 동반한 성인 및 소아에서 topiramate만 추가 병용요법 및 lamotrigine에 대한 연구 3편[52-54]과 levetiracetam에 대한 2편[55,56]의 연구가 평가되었다.
(1) Lamotrigine
만 2-55세 환자를 대상으로 한 1편의 Class II 연구에서 약물난치성 전신 강직간대성 발작을 치료하기 위해(연령 및 추가로 사용한 AEDs의 종류에 따라) 다양한 용량의 lamotrigine과 위약을 비교하였다[54]. 12주간의 전신 강직간대성 발작 빈도 감소율 중앙값과 반응률은 lamotrigine으로 무작위 배정된 환자에서 유의하게 높았다. 가장 흔한 lamotrigine 관련 부작용에는 어지럼, 졸음, 구역이 포함되었다. 두 번째 Class II 연구[52]에서는 증량기와 유지기 동안 baseline 대비 전신 강직간대성 발작 감소율 중앙값에서 lamotrigine에 대해 유의한 차이를 입증하였다. 투여 중단을 초래하는 부작용은 드물었으며, 발진은 보고되지 않았다.
청소년과 성인을 대상으로 서방형 lamotrigine (LTG-XR)을 사용한 Class I 연구에서도 비슷한 결과가 확인되었다[53]. LTG-XR 투여군에서 매주 전신 강직간대성 발작 빈도의 감소율 중앙값이 유의하게 감소하였으며 높은 반응률을 보였다. LTG-XR로 인한 가장 빈번한 부작용에는 오심, 구토, 복시가 있었다.
Recommendation
Lamotrigine 서방형 제제와 속효성 제제(LTG-XR & LTG-IR) 모두 약물난치성 전신 강직간대성 발작에 대한 추가 병용요법이 효과적일 수 있다. (LTG-XR: 1편의 Class I, Level B; Moderate; LTG-IR: 2편의 Class II, Level B; Moderate)
(2) Levetiracetam
2편의 Class I 연구에서 약물난치성 전신성 뇌전증에 대해 levetiracetam 3,000 mg/day와 위약을 비교하였다. 만 4-65세의 환자들이 포함된 연구[54]에서 levetiracetam은 반응률 및 전신 강직간대성 발작 빈도 억제에서 유의하게 높은 소견을 보였다. 다른 연구에서는 청소년 간대성 근경련 뇌전증(JME) 또는 소발작(absence)을 동반한 청소년과 성인을 평가하였다[55]. 위약 대비 levetiracetam 투여군에서 유의하게 더 많은 환자가 간대성 근경련 발작이 나타난 일수가 50% 넘게 감소하여, 간대성 근경련 발작이 없어지고 모든 유형의 발작이 소실되었다. 첫 번째 연구에서는 위약군에서 부작용으로 인한 치료 중단이 더 많았으며, levetiracetam 투여군에서 신경과민, 피로감, 졸음, 두통이 발생하였다. 두 번째 연구에서 levetiracetam 투여 환자에서 더 빈번하게 나타난 부작용은 졸음과 경부 통증, 두 가지뿐이었다.
(3) 성인 및 소아 전신성 발작 난치성 뇌전증에서의 부가요법: 결론
전신성 뇌전증으로 인한 약물난치성 전신 강직간대성 발작을 동반한 성인에서 발작 빈도를 감소시키기 위한 추가 병용요법으로 lamotrigine 속효성 및 서방형 제제를 고려해야 한다(Level B). Levetiracetam은 약물난치성 전신 강직간대성 발작과 약물난치성 청소년 간대성 근경련 뇌전증(JME)에서 발작 빈도 감소를 위해 고려해야 한다(Level B).
2) 레녹스-가스토증후군을 동반한 성인 및 소아에서 부가요법
Lamotrigine, topiramate, clobazam 및 rufinamide가 레녹스-가스토증후군의 치료에 효과적인 것으로 확인되었다. 새로 확인된 임상에서 cannabidiol에 대한 연구가 발표되었다.
(1) Cannabidiol
드라베증후군(영아기 중증 근간대성 뇌전증)과 레녹스가스토증후군(소아기 뇌전증성 뇌병증)의 치료제로 2019년 희귀의약품센터 통한 보급을 식약처에서 승인받았다. Cannabidiol의 작용기전은 잘 알려져 있지 않으며 cannabinoid 수용체 1과 2에 모두 결합하지 않는 것으로 보아 이외의 경로를 통할 것으로 예상된다. 임상 연구에서 clobazam의 대사물인 N-desmethyl clobazam의 농도를 의미 있게 증가시키는 것으로 알려졌다. 이를 통해 항뇌전증효과가 증강되기도 하나 졸음, 쳐짐 등의 부작용도 증가되는 것으로 보인다[6,7].
두 편의 Class I 연구는 위약 대비 cannabidiol을 비교하였다. 하나의 Class I 임상에서 cannabidiol군(10, 20 mg)은 위약군을 비교하였고[57], 다른 하나의 Class I 임상에서 위약 대비 cannabidiol군(20 mg)에서 위약군을 비교하였다. 두 임상에서 cannabidiol군이 위약군 대비 치료 기간 및 유지 기간에서 무긴장성 발작(drop seizure)의 빈도 중앙값이 유의하게 감소하였다. 또한 50% 반응률 역시 위약 대비 유의하게 높은 달성률을 보였다. 가장 흔한 부작용은 두 임상에서 공통되게 졸음, 식욕저하, 설사였고, 두 번째 임상에서는 추가로 발열과 구토가 보고되었다[58]. 일부 cannabidiol군(9%)에서는 간효소 수치가 증가하였다[57].
Recommendation
Cannabidiol은 레녹스-가스토증후군에 대한 추가 병용요법으로 효과적이다. (2편의 Class I, Level A; Strong)
(2) Clobazam
위약 대비 clobazam의 유효성은 2편의 Class II 연구에서 비교하였으며, 3가지 하루 용량(0.25, 0.5, 1 mg/kg)을 조사하였다[15,16]. 세 용량 모두 1주일 동안 무긴장성(drop) 발작 발생률이 baseline 발작 빈도와 비교하여 유의하게 감소하였고, 고용량군일수록 큰 감소를 보였다. 긴장성 발작도 용량의존적으로 감소하였다. 가장 흔한 부작용은 졸음, 무기력, 진정, 침 과다분비, 변비, 폭력성, 조증, 불면증이 포함되었다. 투여 중단을 초래한 가장 빈번한 부작용은 무기력, 폭력성, 운동실조, 피로감 및 공격성이 있었다.
Recommendation
Clobazam은 레녹스-가스토증후군에 대한 추가 병용요법으로 효과적일 수 있다. (2편의 Class II, Level B; Moderate)
(3) Rufinamide
2편의 Class I 연구에서 소아 및 연령대가 낮은 성인을 대상으로 rufinamide과 위약을 비교하였다[17,18]. 최대 45 mg/kg/day의 용량까지 조사하였다. Rufinamide로 무작위 배정된 환자에서 전체 발작 빈도와 무긴장성 발작 빈도의 감소율 중앙값이 유의하게 큰 소견을 보였고, 강직-무진장성(tonic-atonic) 변화율의 중앙값이 더 큰 소견을 보였다. 흔한 부작용으로 졸음, 구토, 식욕 감소가 포함되었다.
Recommendation
Rufinamide는 레녹스-가스토증후군에 대한 추가 병용요법으로 효과적이다. (2편의 Class II, Level B; Moderate)
(4) 레녹스-가스토증후군: 결론
레녹스-가스토증후군에서 발작 빈도를 낮추는 추가 병용요법으로 cannabidiol, rufinamide를 고려해야 하며(Level A), clobazam 사용도 고려해야 한다(Level B).
3) 드라베증후군을 동반한 소아 환자에서 부가요법
Cannabidiol에서 두 편의 Class I 임상이 확인되었다[59,60]. 하나의 Class I에서 소아 및 젊은 성인(~18세) 대상으로 cannabidiol군(20 mg/kg/day)이 위약 대비 월별 발작 횟수 중앙값의 유의한 감소를 보였고, 50% 발작 감소 달성률 및 무발작 비율이 유의하게 높았다. Cannabidiol군에서 탈락비율이 높았으며, 간기능검사에서 이상이 보고되었다[59]. 다른 하나의 Class I에서 소아 및 젊은 성인(~18세) 대상으로 cannabidiol군(10 혹은 20 mg/day)이 위약 대비 발작 횟수의 유의한 감소를 보였다. Cannabidiol 20 mg이 10 mg 보다 간효소 수치가 증가한 것으로 보고되었는데 이는 발프로산(valproic acid)의 병용으로 인한 것으로 보인다[60]. 두 임상에서 cannabidiol의 흔한 부작용 발생으로는 공통적으로 살사, 피로, 발열, 졸음이었고 구토가[59,60] 추가로 확인되었다. 또한 간기능(ALT) 이상이 보고되었다.
Recommendation
드라베증후군에서 발작 빈도를 낮추는 추가 병용요법으로 cannabidiol이 효과적이다. (2편의 Class I, Level A; Strong)
4. 소아 난치성 국소 뇌전증에서의 부가요법
기존 연구에서 gabapentin, lamotrigine, oxcarbazepine 및 topiramate가 효과적이라고 알려져 왔다[53]. 이후로 다음과 같은 8편의 연구가 발표되었다: levetiracetam에 대한 연구 3편, oxcarbazepine에 대한 연구 1편, zonisamide에 대한 연구 1편, perampanel 1편, lacosamide 1편, eslicarbazepine 1편이었다[5]. 새로 확인된 임상은 perampanel, eslicarbazepine, lacosamide, levetiracetam은 각 한 편이었다.
1) Perampanel
한편의 Class III 임상에서 perampanel군(8, 12 mg/day)이 위약 대비 부분 발병 발작의 경우 28일간 발작 빈도 감소 중앙값 및 SG 발작에서 유의하게 감소되었다. 일차성 전신 강직간대성 발작에서는, 위약군 대비 perampanel (8 mg/day)에서 더 높은 28일당 발작 감소 중앙값 및 무발작률을 보였다. Perampanel군에서 가장 흔한 부작용으로는 현기증, 졸음, 두통 및 비인두염이 보고되었다[61].
2) Eslicarbazepine
한 편의 Class I 임상에서 eslicarbazepine (10-30 mg/kg/day)이 위약 대비 standardized seizure frequency (SSF)와 proportion of responders (≥50% SSF reduction) 수치상으로 각각 개선된 결과를 보였다. Post-hoc analysis에서 6세 이상 환자에서는 위약군 대비 eslicabazepine 30 mg/kg/day에서 유의하게 SSF의 감소를 보였다. 가장 빈번하게 보고된 부작용으로는 두통, 비인두염과 졸음이었다[62].
Recommendation
Eslicarbazepine은 소아ㆍ청소년의 국소 난치성 뇌전증에 대한 추가 병용요법으로 효과적일 수 있다. (Class I, Level B; Moderate)
3) Lacosamide
한편의 Class I 임상에서 lacosamide를 체중에 따라 적절히 증량한 치료 약물군이 위약 대비 유의하게 28일간 부분발작 감소율을 보였으며, 50% 반응률 역시 lacosamide에서 유의한 반응을 보였다. 가장 흔한 부작용은 졸음과 어지럼이었다[63].
Recommendation
Lacosamide는 소아ㆍ청소년의 국소 난치성 뇌전증에 대한 추가 병용요법으로 효과적일 수 있다. (Class I, Level B; Moderate)
4) Levetiracetam
2편의 Class I 연구에서 levetiracetam과 위약을 비교하였다. 첫 번째 연구[20]에서는 소아 및 연령대가 낮은 청소년(만 4-16세)을 대상으로 하였으며 목표 용량은 60 mg/kg/day였다. Levetiracetam 투여군에서 일주일간 치료 반응률 및 발작 빈도 감소율 중앙값이 유의하게 큰 소견을 보였다. Levetiracetam 투여군에서 부작용이 더 빈번하였고, 이러한 부작용으로는 졸음, 사고로 인한 상해, 구토, 식욕부진, 비염, 적개심, 기침, 인두염 및 신경질이 포함되었다. 그러나 부작용으로 인한 중도 탈락은 위약에 배정된 소아에서 더 많았다. 두 번째 Class I 연구에서는 생후 1개월부터 만 4세 미만의 무작위 배정된 소아를 대상으로 생후 6개월 미만이면 40 mg/kg/day, 생후 6개월 이상이면 50 mg/kg/day 용량의 levetiracetam과 위약을 비교하였다[21]. Levetiracetam으로 무작위 배정된 소아에서 하루 평균 발작 빈도에 대한 반응률과 baseline 대비 발작 빈도 감소율 중앙값이 더 큰 소견을 보였다. 가장 빈번하게 보고된 부작용에는 졸음과 신경과민이 포함되었다.
한 편의 Class III 임상이 새로 확인되었다. 브라질에서 성인 및 약 45% 이상 소아가 포함된 임상으로, 50% 반응률에서 levetiracetam군(1,000-3,000 mg/day)에서 주당 발작 횟수에 따른 50% 발생률이 위약군 대비 유의하게 높았다. 위약군과 유사한 안전성이 확인되었으며, 상위 3개의 부작용은 신경계, 감염, 위장관계 증상이었다[14].
Recommendation
Levetiracetam은 소아ㆍ청소년의 난치성 국소 뇌전증에 대한 추가 병용요법으로 효과적일 수 있다. (1편의 Class I, Level B; Moderate) 또한 levetiracetam은 영아 및 만 4세 미만의 소아의 약물난치성 국소 뇌전증에 대한 추가 병용요법으로 효과적일 수 있다. (1편의 Class I, 1편의 Class III, Level B; Moderate)
5) Oxcarbazepine
생후 1개월부터 만 4세 미만의 소아를 대상으로 한 Class I 연구에서 2가지 용량(10 및 60 mg/kg/day)의 oxcarbazepine을 비교하였다[21]. 일차 결과변수는 3일 연속 투여 동안 검사한 뇌파에서 24시간 단위당 국소 발작 빈도수의 baseline 대비 절대값 변화였다. 저용량보다 고용량 oxcarbazepine을 투여한 소아에서 발작 빈도 감소가 유의하게 큰 것으로 나타났고, 24시간 동안 발작 빈도 감소율 중앙값도 더 큰 것을 확인할 수 있었다. 고용량을 투여한 소아군에서 졸음, 운동실조 및 구토와 같은 부작용을 더 빈번하게 경험하였다.
Recommendation
Oxcarbazepine은 영아 및 연령대가 낮은 소아의 치료-저항성 국소 뇌전증에 대한 추가 병용요법으로 효과적일 수 있다. (1편의 Class I, Level B; Moderate) 그러나 연구 기간이 짧았다는 점을 감안해볼 때, 일반화에는 제한이 있을 수 있다.
6) Zonisamide
소아 및 만 6-17세 청소년을 대상으로 한 Class I 연구에서 zonisamide 8 mg/kg/day와 위약을 비교하였다[22]. 12주차에서의 반응률은 zonisamide로 무작위 배정된 환자에서 유의하게 높았다. 두 군 간 부작용 발생률에는 차이가 없었으나 위약군에서 부작용으로 인한 탈락이 더 자주 발생하였다. Zonisamide 투여군에서 더 빈번하게 나타난 부작용은 식욕 감소, 체중 감소, 졸음, 구토, 설사가 있었다.
Recommendation
Zonisamide는 소아ㆍ청소년의 국소 약물난치성 뇌전증에 대한 추가 병용요법으로 효과적일 수 있다. (1편의 Class I, Level B; Moderate 및 2편의 class II; Level B; Moderate) 이 환자군에 대한 추가 병용요법으로 clobazam, perampanel, pregabalin, rufinamide, vigabatrin의 유효성에 관한 데이터는 입수되지 않았다.
7) 소아 난치성 국소 뇌전증에서의 부가요법: 결론
발작 빈도 감소를 위해 levetiracetam을 고려해야 하며(생후 1개월부터 만 16세에서 Level B), zonisamide도 고려해야 한다(만 6-17세에서 Level B). 또한 발작 빈도 감소를 위해 oxcarbazepine도 사용해 볼 수 있다(생후 1개월부터 만 4세에서 Level B). 이들 소아ㆍ청소년에 대한 추가 병용요법으로 clobazam, eslicarbazepine, lacosamide, perampanel, pregabalin, rufinamide, vigabatrin의 유효성에 관한 근거는 확인되지 않았다(Level U).
5. 요약
1) Vigabatrin, pregabalin, lacosamide, rufinamide, perampanel, cenobamate, eslicarbazepine, brivaracetam은 성인 약물난치성 뇌전증 환자의 부가요법으로 효과적일 수 있다(Level A; Strong).
2) Topiramate-ER와 pregabalin-ER은 성인 약물난치성 국소 뇌전증 환자의 부가요법으로 효과적일 수 있다(Level B; Moderate).
3) Levitiracetam과 clobazam은 약물난치성 국소 뇌전증 환자의 부가요법으로 효과적일 수 있다(Level C; Weak).
4) 최근 발매된 뇌전증약의 하나인 brivaracetam은 5개 이상의 뇌전증약에 실패한 성인 약물난치성 국소 뇌전증 환자에게 부가요법으로 효과적일 수 있다(Level C; Weak).
5) Eslicarbazepine은 성인 약물난치성 국소 뇌전증 환자의 빌작 빈도를 감소시키기 위해 단독요법으로 고려해 볼 수 있다(Level C; Weak).
6) Lamotrigine IR과 ER은 성인 약물난치성 전신 강직간대성 발작을 동반한 뇌전증 환자의 부가요법으로 고려해 볼만하다. Levetiracetam은 성인 약물난치성 전신 강직간대성 발작을 동반한 뇌전증 환자와 약물난치성 청소년 근간대 뇌전증(JME)의 부가요법으로 사용할 수 있다(Level B; Moderate).
7) Cannabidiol과 rufinamide는 레녹스-가스토증후군의 부가요법에 효과적이다(Level A; Strong).
8) Clobazam 역시 레녹스-가스토증후군의 부가요법에 효과적이다(Level B; Moderate).
9) Cannabidiol은 드라베증후군의 부가요법으로 효과가 있다(Level A; Strong). Levetiracetam은 생후 1개월에서 16세 사이, zonisamide는 6세에서 17세 사이, oxcarbazepine은 생후 1개월에서 4세 사이의 소아 약물난치성 뇌전증 환자에게 부가요법으로 고려할 수 있다(Level B).
결 론
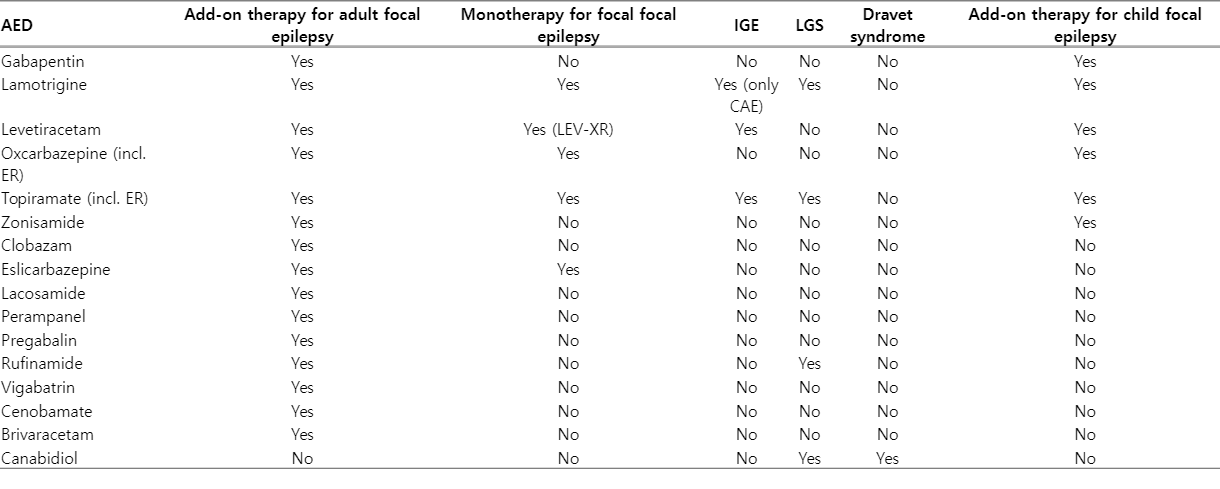
대한신경과학회는 2015년 대한뇌전증학회가 제안한 뇌전증 약물 치료지침과 그 이후 국내에서 사용 중이거나 식약처의 허가를 받았거나 혹은 곧 도입 예정인 뇌전증약의 약물난치성 뇌전증 환자를 대상으로 한 연구 문헌을 검토하여 다음과 같이 약물난치성 뇌전증 환자에서의 뇌전증약 사용 권고 혹은 지침을 제시한다(Table 4).

Recommendations for drug refractory epilepsy patients
본 진료지침 또는 권고 사항을 통해 약물난치성 뇌전증 환자를 치료함에 있어 기존 뇌전증약과 새롭게 도입되는 뇌전증약을 적절히 사용함으로써 다양한 뇌전증 환자에 대한 좀 더 전문적이고 효과적인 치료 접근에 도움을 받기 바란다. 지금 권고사항은 당연히 최종 결론은 아니며, 추후 새로운 정보의 추가 및 뇌전증약의 개발에 따라 꾸준히 갱신되어야 할 것이다.