

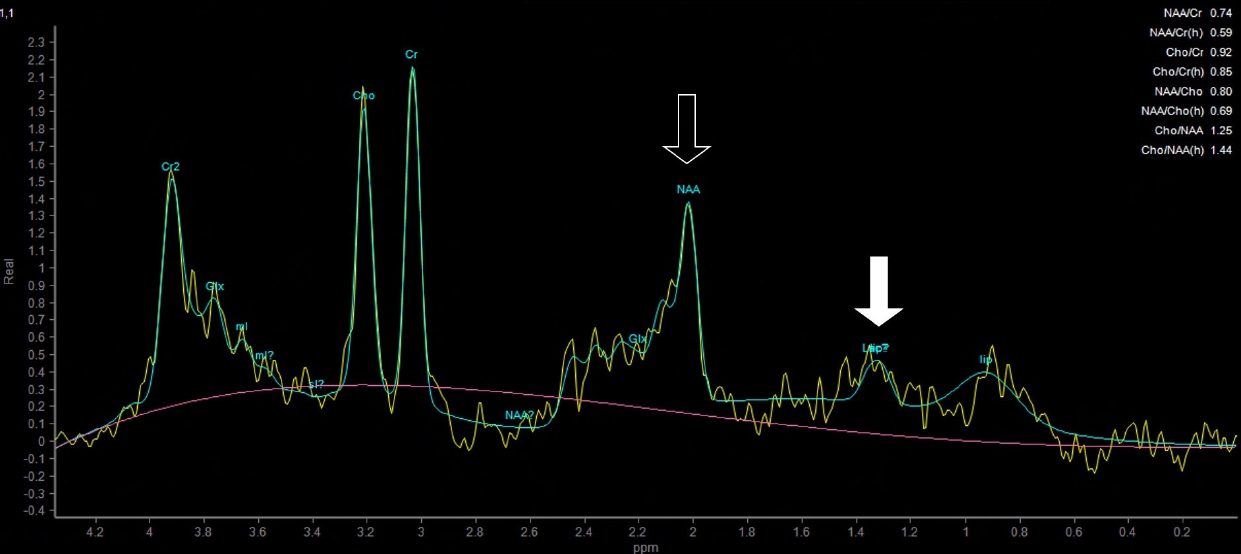
29세 남자가 3주 전부터 발생한 발작으로 왔다. 좌측 시야의 반짝거림으로 시작해 멍해지는 발작이 반복적으로 발생하였으며, 좌측 동측반맹이 보였다. 혈당 362 mg/dL, 당화혈색소 14.6%였고 뇌 magnetic resonance imaging (MRI)에서 비케톤고혈당유발발작에서 관찰되는 소견이 있었다(Fig. 1) [1]. 자기공명분광(magnetic resonance [MR] spectroscopy)에서는 젖산 증가와 N-아세틸아스파트산(N-acetyl aspartate, NAA) 감소를 보였다(Fig. 2). 항뇌전증제 사용 없이 혈당 조절 만으로 경련은 즉시 호전되었으며 좌측 반맹은 2주 후 호전되었다.
| J Korean Neurol Assoc > Volume 39(2); 2021 > Article |

|
REFERENCES
1. Lee EJ, Kim KK, Lee EK, Lee JE. Characteristic MRI findings in hyper glycaemia-induced seizures: diagnostic value of contrast-enhanced fluid-attenuated inversion recovery imaging. Clin Radiol 2016;71:1240-1247.


2. Zhu H, Barker PB. MR spectroscopy and spectroscopic imaging of the brain. Methods Mol Biol 2011;711:203-226.

Figure 1.
Brain magnetic resonance images. (A) FLAIR images show the subcortical hypointensity in the right occipital area (arrows) with overlying cortical hyperintensity and gyral swelling. (B) Diffusion-weighted images show cortical high signal intensity (empty arrows) and (C) the ADC maps show low signal intensity in the corresponding area. (arrowheads). FLAIR; fluid attenuated inversion recovery, ADC; apparent diffusion coefficient.

- TOOLS
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print


-
METRICS

-
- 0 Crossref
- 0 Scopus
- 1,076 View
- 46 Download
-

- Related articles
-
Magnetic Resonance Spectroscopy Finding in a Patient with Cerebral Fat Embolism2014 ;32(4)
Aphasic Seizure as a Manifestation of Non-Ketotic Hyperglycemia2012 ;30(4)
In Vivo Proton Magnetic Resonance Spectroscopic Findings in Brain Abscess: A Case Report2007 ;25(3)
- Editorial Office
-
(ZIP 03163) #1111, Daeil Bldg, 12, Insadong-gil, Jongno-gu, Seoul, Korea
Tel: +82-2-737-6530 Fax: +82-2-737-6531 E-mail: jkna@neuro.or.kr
Copyright © 2024 by Korean Neurological Association.

