진단되지 않은 근육병 환자를 대상으로 시행한 늦은 발병 폼페병의 다기관 표적집단선별검사
Multicenter Targeted Population Screening of Late Onset Pompe Disease in Unspecified Myopathy Patients in Korea
Article information
Trans Abstract
Background
Pompe disease is a rare autosomal recessive disorder caused by the deficiency of a lysosomal enzyme, acid alpha-glucosidase (GAA). Early diagnosis and initiation of treatment with enzyme replacement therapy have remarkable effects on the prognosis of Pompe disease. We performed the expanded screening for late onset Pompe disease (LOPD) at eight centers in Korea.
Methods
From September 1, 2015, GAA activity were measured from both dried blood spot (DBS) and mixed leukocyte for 188 available patients. For 12 patients with low GAA activity, we performed Sanger sequencing of GAA gene.
Results
Among 188 patients, 115 were males. The mean of age of symptom onset and diagnosis were 34.3 years and 41.6 years. Among 12 patients with decreased GAA activity, two patients were confirmed to have LOPD with genetic test (c.1316T>A [p.M439K] + c.2015G>A [p.R672Q], c.1857C>G [p.S619R] + c.546G>C [leaky splicing]). Other two patients had homozygous G576S and E689K mutation, known as pseudodeficiency allele.
Conclusions
This study is expanded study of LOPD screening for targeted Korean population. We found two patients with LOPD, and the detection rate of LOPD is 1.06%. With application of modified GAA cutoff value (0.4), which was previously reported, there were no false positive results of GAA activity test using DBS. Therefore, it could be an appropriate screening test for LOPD in especially East-Asian population, in which pseudodeficiency allele is frequent.
서 론
폼페병(Pompe disease, OMIM 232300; 2형 당원축적병[glycogen storage disease type II])은 대사근육병(metabolic myopathy) 중 하나로 용해소체(lysosome) 내에 위치하는 당원을 분해하는 효소인 산성 엿당분해효소(acid maltase, acid alpha 1,4-glucosidase, GAA)가 결핍되어 용해소체 내에 당원이 축적되고 세포사를 일으켜 주로 골격근, 심근, 간 등의 손상을 유발하는 보통염색체 열성 질환이다[1]. GAA 결핍 정도, 유전자형에 따라 임상양상이 다르게 나타나며 발병 시기에 따라 크게 영아발병 폼페병(infantile onset Pompe disease, IOPD), 늦은발병 폼페병(late onset Pompe disease, LOPD)으로 나눌 수 있으며, GAA 효소활성도는 IOPD에서 가장 낮게 측정된다. IOPD의 경우 특징적인 심장, 간비대가 관찰되고 적절한 치료를 하지 않으면 심장기능부전과 호흡마비로 생후 2년 이내에 사망한다[2]. LOPD는 다리와 몸통 근육의 쇠약을 시작으로 병이 진행하면서 얼굴, 혀, 척추주변, 몸통 근육의 쇠약이 뚜렷하면서 호흡곤란이 생기고 식사를 하기 힘든 임상양상을 보인다[1].
폼페병에 대한 치료로 부족한 효소를 정맥으로 주사하여 대체하는 효소대체요법(enzyme replacement therapy, ERT)이 2000년대 이후 IOPD와 LOPD 환자에게 적용되었다. LOPD 환자를 대상으로 진행한 무작위 연구에서 6분 걷기에서 거리가 증가하였고, 호흡기능의 악화를 막았으며[3], 한국에서 ERT를 시행하고 후향적으로 분석한 보고에서도 비슷한 결과를 확인할 수 있었다[4]. 그러나 LOPD의 경우 다른 선천근육병에 비하여 호흡근 마비가 근육 쇠약 정도보다 조금 이른 경향이 있는 것을 제외하고는 팔다리이음근디스트로피(limb girdle muscular dystrophy) 등과 같이 몸쪽 근육 쇠약이 뚜렷한 병과의 구분이 힘들어 진단이 늦는 경우가 많았다[5]. 따라서 신생아를 대상으로 하는 선별검사 혹은 늦은 발병의 경우 진단되지 않은 근육병 환자들을 대상으로 선별검사를 진행하여 치료를 받도록 환자를 찾기 위한 노력을 기울이게 되었다. 신생아를 대상으로 전체 선별검사를 하여 빠른 진단을 할 경우 병의 예후가 더 좋으며[6], 그렇지 못한 경우라도 의심되는 환자에게 선별검사를 시행, 빠른 진단을 하고 치료를 시작하는 것이 중요하다[7-9]. 진단이 되지 않은 근육병이나 근위부 쇠약, 원인 모르는 혈중 크레아틴인산화효소(creatine kinase, CK) 증가 등이 있을 때 LOPD에 대한 선별검사를 진행한 연구에 대한 결과들이 2013년 이후로 발표되었고, 연구 결과를 고려할 때 LOPD 선별검사를 원인을 모르는 근위부 쇠약을 보이는 근육병 환자나 원인을 모르는 혈중 CK의 지속적 증가가 있을 때 시행하고 이상이 보이면 폼페병에 대한 유전자검사가 권장되고 있다. 특히, 위양성 대립유전자(c.1726G>A[p.G576S], c.2065G>A[p.E689K])의 빈도가 높은 아시아인은 GAA 활성도가 낮게 나오더라도 위양성 대립유전자로 인하여 활성도가 낮게 나올 수 있어서 유전자검사를 통한 병적변이의 확인이 중요하다[10,11].
본 저자가 발표했던 한국인 90명을 대상으로 진행한 이전 연구에서 2명을 발견하였으며, 당시 GAA 활성도가 떨어진 14명이 위양성대립유전자를 가지고 있는 것을 알게 되어 한국인도 대만, 중국, 일본 등과 같이 위양성대립유전자의 빈도가 높을 것으로 생각되어 GAA 활성도에 이은 유전자검사가 매우 중요함을 알 수 있었다. 그러나 연구 대상이 90명으로 소수였고, 일부 지역에서만 연구가 진행되어 전국에서 더 많은 다수의 사람들을 대상으로 연구를 진행할 필요성이 있었으며, 위양성대립유전자가 많은 아시아인 한국에서 GAA 활성도의 기준 수정의 필요성에 대한 연구를 위하여 한국에서 신경근육센터가 있으며 참여 가능한 전국의 병원들을 대상으로 연구를 진행하였다.
대상과 방법
1. 환자 등록과 임상데이터 추출
2015년 9월 1일부터 2018년 10월 31일까지 한국의 8개 병원(강남세브란스병원, 부산대학교병원, 서울대학교병원, 서울아산병원, 서울삼성병원, 양산부산대학교병원, 전남대학교병원, 칠곡경북대학교병원[가나다순])의 신경근육센터에서 진단되지 않은 근육병 환자 226명을 전향적으로 등록하여 진행하였다.
환자 등록기준은 아래와 같다: 1) 발병 연령이 12개월 이상; 2) LOPD를 의심할 수 있는 하위 5가지 중 한 가지 이상의 임상양상을 보인 경우: (1) 몸쪽 근육 쇠약(proximal muscle weakness), (2) 몸통 근육 쇠약(axial muscle weakness), (3) 혀 쇠약(lingual weakness), (4) 호흡곤란(respiratory difficulty), (5) 특발지속 혈중 CK 과다 (idiopathic persistent hyperCKemia [hyperCKemia]); 3) 환자 혹은 환자의 법적 대리인의 동의를 구두 혹은 서면으로 받은 경우.
제외기준은 아래와 같다: 1) 추적검사에서 유전학적 혹은 병리학적 검사 결과 다른 신경근육질환이 강하게 의심되거나 확진되는 경우; 2) 환자 가족력에서 보통염색체 우성 혹은 성염색체관련 유전양상을 보이는 경우.
환자의 임상양상, 병력, 검사 소견은 정해진 양식에 따라 수집되었다. 등록기준과 제외기준 재확인과 아래에 소개되는 검사를 모두 제대로 진행한 188명의 임상데이터로 분석을 진행하였다.
환자 등록, 검사 방법 등에 대한 절차는 헬싱키 선언에 기초하여 만들어졌고, 각 병원의 기관윤리심의위원회(Institutional Review Board)의 검토를 거쳐 승인 후 진행되었다.
2. 선별검사 절차
1) 산성 알파 1,4 포도당화물분해효소(acid alpha-1,4-glucosidase [GAA]) 활성도 평가
강남세브란스병원과 양산부산대병원에서 진행되었던 이전 연구와 동일한 방법으로 진행되었다[12]. GAA 활성도를 확인하기 위해서 건조혈액샘플(dried blood spot, DBS)과 혼합백혈구(mixed leukocyte, ML)를 사용하는 방법을 사용하였다. 두 가지 샘플에 4-methyl-umbelliferyl-α-D-glucopyranoside를 사용하여 확인할 수 있는 GAA (tGAAa)는 일부 GAA 활성도 값에 영향을 줄 수 있는 효소들(설탕동종엿당분해효소[sucrose isomaltase], 엿당분해효소-포도당녹말분해효소[maltase-glucoamylase], 2형 포도당화물분해효소[glucosidase II], 중성알파포도당화물분해효소[neutral alpha glucosidase])이 영향을 줄 수 있다[13]. 그래서 아카보오스(acarbose, 알파포도당화물분해효소억제제[alpha glucosidase inhibitor])를 처리하여 순수한 GAA 활성도(GAAa)를 확인하여 그 비율(tGAAa/GAAa, GAA비율)을 구한다. 각 수치의 정상범위는 다음과 같다. DBS: tGAAa: 4.50-27.15 nmol/punch/hr, GAAa: 1.90-7.45 nmol/punch/hr, GAA비율: 0.20-0.85; ML: tGAAa: 17.4-40.4 nmol/mg protein/hr, GAAa: 7.7-20.1 nmol/mg protein/hr, GAA비율: 0.46-0.96.
GAA 활성도 저하의 기준 역시 이전 연구와 동일하게 GAAa와 GAA비율 중 하나가 DBS나 ML 모두 떨어져 있는 경우로 하였다.
2) GAA 유전자검사
유전자검사는 GAA 활성도가 떨어진 환자들에게 진행하였고, 방법은 이전 연구에서 사용한 방법으로 진행하였다[12].
3. 통계분석
통계분석은 SPSS 소프트웨어 버전 24 (SPSS Inc, Chicago, IL, USA)를 사용하여 진행되었다. 기술통계량은 데이터별로 정규성 분포에 따라 표준편차와 평균, 사분범위와 중앙값으로 표현하였다. LOPD 환자와 위양성대립유전자를 지닌 환자 간의 GAA 활성도의 비교를 위해서 Mann-Whitney U test를 진행하였고, p값은 0.05 미만을 통계적으로 의미 있는 것으로 보고 분석하였다.
결 과
연구에 등록된 226명 중 DBS와 ML 샘플 모두 GAA 활성도 검사가 된 경우는 188명이었다. 188명을 대상으로 결과를 분석하였다. 115명이 남자였고, 평균 나이는 41.6세, 증상이 시작된 평균 나이는 33.3세였다. LOPD 관련증상으로 몸쪽 근육 위약은 161명으로 대부분의 환자가 보이고 있으며, 몸쪽 근육 위약이나 호흡곤란, hyperCKemia만 보이는 경우는 각각 1명(0.5%), 3명(1.6%), 20명(10.6%)이었다. 심장기능이상은 27명(14.4%)에서 관찰되었다. 혈중 CK 수치는 평균 1,392 IU/L로 관찰되었다(Table 1).

Baseline characteristics of 188 unspecified myopathy patients
12명의 환자가 GAA 활성의 감소를 보였고, 이후 시행한 유전자 검사에서 2명이 진단되고 나머지 10명 중 6명에게서 동형접합(homozygous) 혹은 이형접합(heterozygous) 위양성대립유전자(pseudodeficiency allele, G576S, E689K)가 관찰되었다. LOPD로 확인된 두 환자에게서 공통적으로 c.1316T>A (p.Met439Lys) 변이가 관찰되었고, 25번 환자는 c.2015G>A (p.Arg67p2Gln), 48번 환자는 c.546G>T (leaky splicing) 변이가 발견되었다. 모두 예전 보고에서 관찰된 병적변이(pathogenic variant)였다(Table 2) [14-16].
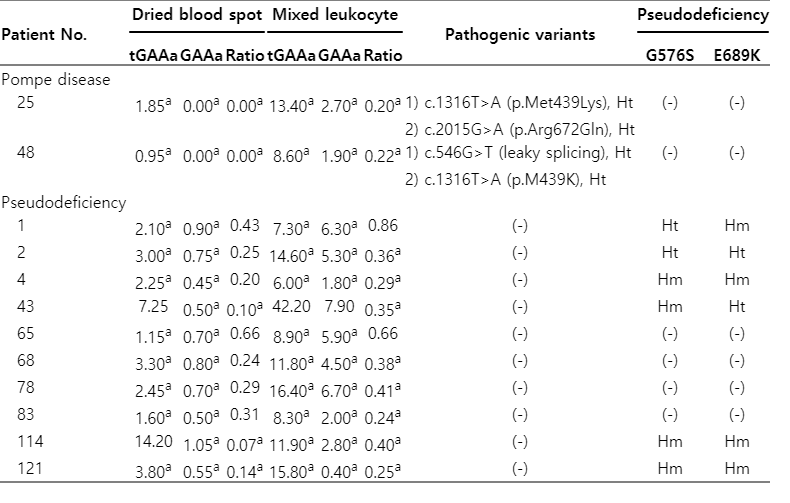
Acid α-1,4-glucosidase (GAA) activity with dried blood spot and mixed leukocyte, and genotypes of 12 patients with decreased GAA activity
LOPD로 진단된 두 명 환자 모두 여자였고, 25번 환자는 40세, 48번 환자는 18세였으나, 증상이 생기기 시작한 나이는 모두 9세였다. 25번 환자의 경우 증상이 생기고 나서 이번 연구에 등록되어 진단되기까지 31년의 긴 시간이 걸렸으며, 현재 거의 잘 움직이지 못하여 침대에 누워 지내고 있는 상태라서 CK도 25번 환자는 약간 올라간 수치이나, 48번 환자의 경우 2,113 IU/L로 정상치의 10배 이상 수치를 보였다. 두 명 모두에게서 침근전도검사에서 폼페병의 특징인 근긴장전위(myotonic discharge)가 관찰되었다(Table 3).

Clinical characteristics of genetically confirmed two late-onset Pompe disease patients
동형접합 위양성대립유전자는 3명에서 관찰되었으며(1.6%), 이형접합 위양성대립유전자를 가진 환자와의 GAA 활성도 차이는 보이지 않았다. 이전 연구와 비슷하게 이번 연구에서도 DBS 샘플에서의 GAAa와 GAA비율은 위양성변이를 가진 환자와 LOPD 환자 간의 차이가 뚜렷하였고(p=0.03), ML 샘플에서는 GAA비율만 통계적인 의미를 보였다. 이전 연구에서 제시하였던 DBS 샘플로 얻는 GAAa 0.4의 값을 적용하면 이번 연구 환자들에게서 위양성인 경우는 없었다[12].
고 찰
LOPD는 서론에서 서술한 바와 같이 현재 치료법으로 사용할 수 있는 약이 있으며, 비교적 쉽게 진단이 가능한 유전병으로 IOPD에 비하여 증상이 다른 신경근육질환으로 오인될 가능성이 높아 빠르고 정확한 진단이 중요하다. 이번 연구를 통하여 대한민국의 각 지역에서 근육병을 진료하고 있는 다양한 신경근육센터에서 진단되지 않는 근육병 환자들 중 LOPD를 의심할 수 있는 증상을 가진 환자들을 대상으로 LOPD 환자를 찾고자 하였다. 서울의 강남세브란스병원과 남부지방의 양산부산대병원에서 진행하였던 지난 연구보다 다양한 지역에서 진행하고 더 많은 수를 대상으로 연구를 진행하여 지역적, 사회적으로 다양한 구성의 환자가 등록되었기 때문에 이번 연구가 보다 더 의미가 있다고 볼 수 있다.
또한 현재까지 폼페병을 진단하는 검사 방법은 혈액, 근육, 섬유모세포 등 다양한 세포들로 진행되었고, 혈액 샘플 중에서는 림프구를 분리하여 시행하는 것이 정확하지만, 검사의 효율성 등을 고려하여 ML 혹은 DBS를 이용하여 GAA 활성도를 확인하고, GAA 활성도의 저하가 관찰되면 GAA 유전자검사를 하여 병적변이를 찾아내는 방식으로 진행하고 있었다[1]. 최근에는 차세대염기서열분석(next generation sequencing, NGS) 기술이 가격도 저렴하고 방법이 쉬워지면서, 유전병이 의심되는 경우 근육병 유전자를 타겟 NGS로 진행하여 찾아내는 방법도 사용하기도 한다[17]. 한국에서 진행한 연구의 경우 ML과 DBS 모두를 한번에 진행하여 GAA 활성도를 여러 번 측정하기 위해 환자가 감수해야 했던 불편과 시간낭비를 줄였다.
이번 연구를 통하여 2명의 LOPD 환자를 찾아 내었다. GAA 활성도 검사가 모두 제대로 진행된 188명 중 2명이 진단된 것으로 진단율은 1.06%였다. 예전 외국에서 진행되었던 연구에서는 0-4.6%의 유병률을 보였다[18-25]. 최근까지 외국에서 진행된 연구들의 경우 초기에는 진단이 되지 않은 근육병 환자들을 대상으로 진행하였으나, 팔다리 몸쪽 쇠약과 무증상의 hyperCKemia와 같은 LOPD의 주요 증상을 가진 환자들을 대상으로 선별검사를 하였다. 한국의 지난 선별검사 연구에서도 2.2%의 진단율을 보였으며[12], 이번 연구에서도 1.06%의 진단율을 보여 예전 외국에서 시행되었던 연구에서의 진단율과 큰 차이는 보이지 않았다. LOPD로 확인된 두 환자에서 공통적으로 c.1316T>A (p.M439K) 변이가 관찰되었고, 25 번 환자는 c.2015G>A (p.R672Q), 48번 환자는 c.546G>T (leaky splicing) 변이가 발견되었다. 모두 예전 보고에서 관찰된 병적변이이다. 공통적으로 관찰된 변이는 c.1316T>A로 이는 한국인에게서 처음 발견되어[15], 이후 IOPD와 LOPD 모두에게서 관찰되고, 비공식집계에서 가장 많이 확인된 변이이다. 25번 환자에게서 관찰된 p.R672Q의 경우 청소년기 발병 폼페병에서 동형접합형으로 발견되었던 변이이다[14]. 그리고 48번 환자에게서 관찰된 변이인 c.546G>T (leaky splicing)는 일본에서 청소년기 발병에서 p.R600C 변이와 함께 이형접합형으로 관찰되었던 변이이며, 이전 선별검사 연구에서 관찰되었던 변이이다[12,16]. 이번에 찾은 두 환자 모두 발병 연령이 9세인 것을 볼 때 예전 보고와 표현형은 비슷하다고 보인다.
위양성대립유전자인 p.G576S, p.E689K가 동형접합으로 있는 경우는 3명이었고, 분석된 188명 중 3명으로 1.6%이다. 지난 연구에서는 6명으로 6.7%에 달해 근처 국가인 일본(3.3%), 대만(3.9%)에 비해 많아 한국인의 특수성일 가능성에 대하여 고민하였으나, 이번에는 1.6% 정도로 다수로 진행하였을 경우 더 적게 나오며, 한국인 참조유전체 연구에서 제공한 Korean Reference Genome Database에 제공된 빈도에 따르면[26], G576S의 빈도가 17.6%이고, 이 변이는 E689K와 항상 같이 나오는 바 동형접합형 위양성대립 유전자를 가진 사람의 빈도를 계산해보면 2.89%로 지난번 연구의 6.7% 빈도는 우연한 결과였던 것으로 생각된다.
이전 연구에서 진행된 데이터를 같이 분석해 보았을 때, DBS를 가지고 측정한 GAA 활성도는 tGAAa, GAAa, GAA비율 모두 환자와 위양성 대립유전자 그룹 간 통계적 의미를 보이고 있으며(p-value: tGAAa, 0.019; GAAa, 0.001; GAA비율, 0.000), ML을 가지고 진행할 때에도 GAAa, GAA비율 모두 통계적 의미를 보인다(p-value: GAAa, 0.001; GAA 비율, 0.000). 그러나 진단검사시 좀 더 경제적인 검사를 위해 GAA 활성도의 기준치를 설정함에 있어 그 두 가지 그룹 간의 차가 큰 것은 DBS를 가지고 한 GAAa였다(DBS-환자: 0-0.05 vs. 위양성대립유전자: 0.4-1.6, ML-환자: 1.4-2.7 vs. 위양성대립유전자: 1.8-9.3). 한 번의 검사로 두 그룹 간의 분명한 차이를 보기 위해서는 DBS가 적당하며, 검사 방법이나 운반 등도 쉽기 때문에 유전자검사 전 선별검사로 위양성대립 유전자의 빈도가 높은 동아시아권 국가, 특히 한국에서는 DBS를 이용한 GAA 활성도를 보는 것이 적절할 것으로 보인다.
한국에서 다수의 진단되지 않은 근육병 환자를 대상으로 연구를 진행하긴 하였으나, 이전 연구의 2배가 조금 넘는 수준으로 GAA 활성도의 기준을 조정할 정도는 아니었다. 그리고 환자와 병원의 사정에 따라 GAA 활성도를 DBS, ML 모두 진행하지 못한 환자들 이 있어 GAA 활성도의 기준을 바꾸기엔 절대적인 수가 부족한면이 있었다. GAA 활성도 기준에 대한 조정을 하기 위해서는 좀 더 많은 환자의 결과가 필요하다고 생각된다. 이전 연구와 데이터를 합쳐서 분석할 경우 환자와 위양성대립유전자를 가진 그룹 간의 차이는 DBS에서 좀 더 뚜렷한 경향을 보이긴 하였으나, 이에 대해서는 좀 더 추가적인 데이터 수집을 통한 분석이 필요할 것으로 생각된다.
전국의 진단되지 않은 근육병 환자 중 폼페병과 관련한 증상을 보이는 환자들을 대상으로 선별검사를 진행할 경우 폼페병을 진단할 가능성을 이번 연구를 통하여 한 번 더 확인할 수 있었고, 근육병이 의심되는 환자의 경우 팔다리의 몸쪽 쇠약과 함께 몸통 근육 쇠약이 명확하거나, 호흡마비가 빠르거나 혀의 위약 등이 보이는 경우, 또는 원인을 알기 힘든 지속적인 hyperCKemia가 관찰되는 경우 폼페병의 가능성이 있으므로 현재 치료, 관리 방법이 있는 폼페병에 대한 선별검사를 고려해야 한다. 그리고 위양성대립유전자의 빈도가 높기 때문에 GAA 활성도의 기준에 대한 추가적인 연구가 필요하다.