알츠하이머병의 새로운 생물학적 정의: 2018 National Institute on Aging-Alzheimer’s Association Research Framework 소개
A New Biological Definition of Alzheimer’s Disease: Introduction of 2018 National Institute on Aging-Alzheimer’s Association Research Framework
Article information
Trans Abstract
Diagnostic guidelines for the preclinical, mild cognitive impairment, and dementia stages of Alzheimer’s disease (AD) were released by the National Institute on Aging and Alzheimer’s Association (NIA-AA) in 2011. Promoted by the subsequent scientific progress, a unifying update, the ‘NIA-AA Research Framework’, was published in 2018. This new research framework shifts the definition of AD from syndrome to biological construct based on biomarkers in living people. The biomarkers were grouped into β amyloid deposition (A), pathologic tau (T), and neurodegeneration (N) related, termed the ‘AT(N) classification system’, which could be extended with new biomarkers as they become available in the future. For the staging of cognitive impairment, three syndromal stages for observational studies and six numeric stages for clinical trials were also suggested. This biomarker-based classification combined with clinical staging is expected to enhance the understanding of AD as well as aid in precise targeting for interventional clinical trials. This review focused on the introduction of the new 2018 NIA-AA Research Framework. Although this framework has been proposed for research purposes, it is expected to be adopted into general clinical practice with thorough examination and validation in the future.
서 론
미국 국립노화연구소(National Institute of Ageing, NIA)와 알츠하이머협회(Alzheimer Association, AA)가 공동으로 2011년에 발표한 NIA-AA 알츠하이머병 진단기준은 임상증상에 기반하여 임상증상 전 알츠하이머병(preclinical Alzheimer’s disease), 알츠하이머병에 의한 경도인지장애(mild cognitive impairment due to Alzheimer’s disease), 알츠하이머병 치매(dementia due to Alzheimer’s disease)로 구분하고 각각에 대한 진단 가이드라인을 제시한 바 있다[1-4]. 생물표지자의 경우는 관찰 연구 및 임상시험 등 연구 목적으로 활용하도록 권고하였고, 병리 기반에 근거하여 베타아밀로이드(β-amyloid, Aβ)의 축적(뇌amyloid-positron emission tomography [PET] 양성 소견, 뇌척수액 Aβ1-42 농도 감소)과 신경퇴행(뇌 fluoro-deoxyglucose [FDG]-PET상 측두엽 및 두정엽 대사 감소, 뇌 magnetic resonance imaging [MRI]상 내측두엽 위축, 뇌척수액 tau 농도 증가)의 두 가지 범주로 구분하였다[4]. 이처럼 신경영상과 뇌척수액에 기반한 생물표지자를 진단기준에 포함시켜 치매 상태뿐만 아니라 증상이 없는 임상증상 전 단계에서도 알츠하이머병을 진단하는데 적극적으로 활용하게 되면서, 알츠하이머병의 인지기능이 지속적으로 악화되는 것과 마찬가지로 생물표지자도 오랜 시간에 걸쳐 증상 발생 이전부터 연속적으로 변화한다는 연구 결과들이 축적되기 시작하였다[5-7]. 이후에, tau-PET의 리간드가 개발되어 임상 및 관찰 연구에서 사용되었고[8,9], 이는 2011년도 진단기준에서는 신경퇴행 생물표지자에 포함되었던 뇌척수액의 과인산화된 타우단백질과 함께 알츠하이머병의 특이 생물표지자로서 인지되면서 기존의 두 개의 범주로 나누었던 생물표지자에 대하여 세분화할 필요성이 제시되었다. 따라서, 최신 연구 결과들을 반영하여 2011년의 NIA-AA 진단기준을 업데이트한 2018년 ‘NIA-AA Research Framework’가 제시되었으며[10], 본 원고에서는 이를 바탕으로 알츠하이머병의 새로운 생물학적 정의를 소개하고 그 의미를 고찰해 보고자 한다.
본 론
1. AD 용어의 정의
‘알츠하이머병(Alzheimer’s disease, AD)’이라는 용어는 신경병리적 변화의 집합을 말하며, 이러한 변화를 생체 내(in vivo) 생물표지자나 사후 병리검사를 통하여 확인한 경우로 정의하였다. 따라서, 기존의 임상증상에 기반하여 정의한 ’probable AD’ 또는 ‘possible AD’이라는 용어는 ‘알츠하이머 임상증후군(Alzheimer’s clinical syndrome)’으로 대체할 것을 권고하였다. 같은 알츠하이머병이라고 하더라도 임상증상은 다양하게 나타날 수 있고[11,12] 생물표지자의 변화에 비하여 증상은 상대적으로 질병이 진행된 후에 나타나게 되므로, 임상증상과 생물표지자를 분리하여 생물표지자의 변화만으로도 알츠하이머병을 정의한 부분은 기존의 임상증상에 기반한 진단기준과 비교하여 상당한 사고의 전환이라고 할 수 있다. 이로 인하여 AD는 특정 증상들에 의한 임상증후군에서 특징적인 병리 기전을 가진 하나의 구체적인 질병이 되었다.
2. ‘AT(N) 분류 체계’를 이용한 AD 생물표지자의 분류
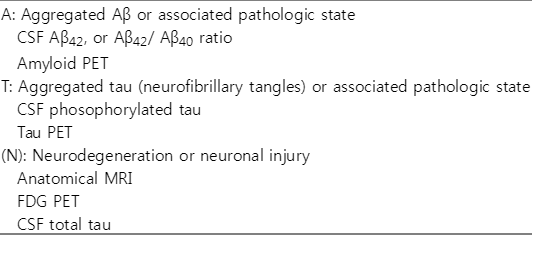
최근 알츠하이머병과 뇌의 노화 연구를 위하여 제안된 소위 ‘AT(N) 분류 체계’를 2018년도 Research Framework의 기본으로 하여 다양한 뇌영상과 뇌척수액 생물표지자 중에서 타당성이 검증된 지표를 채택하였다(Table 1) [13]. 즉, 생물표지자 분류를 크게 3개의 범주로 나누었는데, ‘A (=Amyloidopathy)’는 베타아밀로이드 관련 지표로 뇌피질의 amyloid-PET 리간드의 결합이나 뇌척수액에서의 Aβ42 (또는 Aβ42/Aβ40)의 감소로 정의하였고[14,15], ‘T (=Tauopathy)’는 신경원섬유매듭 형태의 타우 관련 지표로 뇌척수액에서의 인산화 타우의 증가나 뇌피질의 tau-PET 리간드의 결합으로 정의하였다[16,17]. ‘(N) (=Neurodegeneration or Neuronal injury)’은 신경퇴행의 지표로 뇌척수액 총 타우의 증가 또는 MRI에서의 뇌위축과 FDG-PET에서의 뇌 대사저하를 포함하고 있다[18-20]. 즉, 현재의 AT(N) 체계는 뇌척수액검사와 뇌영상 생물표지자를 이용하여 각각 아밀로이드병증(A), 병적 타우(T), 신경퇴행(N)의 여부를 파악하고 이를 질병 정의에 활용하였다. 연구 그룹에 따라서 뇌척수액과 뇌영상 두 범주에 해당하는 생물표지자를 각각 사용하거나 경우에 따라서는 함께 사용하는 것도 가능하다[13].
3. 생물표지자에 의한 질병의 정의 및 범주
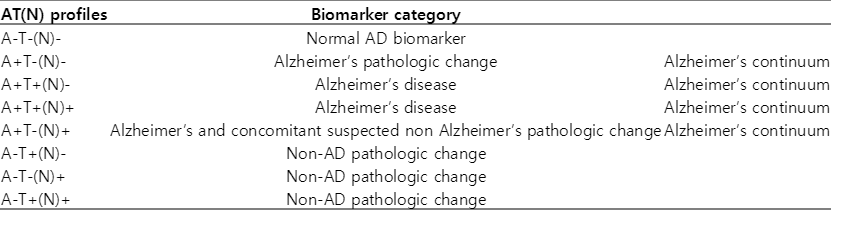
2018 Research Framework 위원회에서는 상술한 AT(N) 생물표지자 분류 체계 중에서 알츠하이머병 특이 지표인 베타아밀로이드와 병적 타우를 반영하는 지표로, 즉 아밀로이드병증(A)과 병적 타우(T)로 알츠하이머병을 정의하기로 결정하였다[21,22]. 대상자가 베타아밀로이드 침착과 관련된 생물표지자의 변화만을 보인다면 ‘알츠하이머의 병적 변화(Alzheimer’s pathologic change)’ 단계이며 병적 타우 지표의 변화까지 확인되면 ‘알츠하이머병(Alzheimer’s disease)’ 단계로 명명하기로 하였다(Table 2). 이 두 가지 단계는 각각 ‘알츠하이머 연속체(Alzheimer’s continuum)’의 초기와 후기 단계로 임상증상에 상관없이 적용하게 된다. 아밀로이드병증(A), 병적 타우(T), 신경퇴행(N)에 해당하는 각각의 생물표지자의 값에 차단점(cut point)을 기준으로 정상/비정상으로 구분하여 총 8개의 경우의 수를 가지는 ‘생물표지자에 따른 분류(biomarker profile)’를 만들었다(Table 2). AT(N) 분류 체계를 이용한 알츠하이머 질병 정의를 고려하면 개개인은 생물표지자 분류에 의하여 알츠하이머 생물표지자의 이상이 없는 정상군(normal AD biomarker)과 Alzheimer’s continuum에 해당하는 경우, 그리고 알츠하이머가 아닌 다른 병리 소견(non-AD pathologic change)을 가지는 3개의 범주 중 하나에 속하게 된다. Alzheimer’s continuum 중 ‘A+T-(N)+’는 ‘알츠하이머 병리 소견과 다른 병리 소견이 섞여 있는 상태(Alzheimer's and concomitant suspected non-Alzheimer's pathologic change)’로서 ‘T’ 생물표지자를 포함하면서 새로이 추가된 개념이라고 할 수 있다. 또한 알츠하이머가 아닌 다른 병리 소견에 해당하는 군은 기존의 ‘suspected non-Alzheimer’s pathophysiology (SNAP)’ [23]에 해당하며, 베타아밀로이드 관련 지표가 음성이면서 하나 이상의 다른 신경병리의 증거가 확인된 군이다.
4. 생물표지자의 특징과 제한점
뇌척수액과 뇌영상 생물표지자가 각각 A, T, (N)의 같은 그룹 내에 분류가 되어 있지만 뇌척수액은 특정한 시점에 병적 단백질이 생성되고 제거되는 속도를 반영한다면, 뇌영상은 시간을 두고 축적된 신경병리 소견을 반영한다. 따라서, 뇌척수액과 뇌영상의 결과가 한 시점에 다르게 나올 수 있는데 알츠하이머병의 만성 진행 양상을 고려한다면 결국 장기적 관점에서는 일치하게 될 것으로 기대할 수 있다[24-26]. 상대적으로 새로운 도구라고 할 수 있는 tau-PET은 많은 초기 리간드가 비특이적 결합(off-target binding)의 문제를 보였다[27]. 초기 리간드 중 flortaucipir는 이러한 비특이적 결합이 적었고 이어서 개발된 새로운 리간드들을 통하여 특이성을 높일 것으로 기대하고 있다[28-30]. 뇌척수액의 인산화 타우와 총 타우의 경우는 인산화 타우가 알츠하이머병에서만 일관되게 증가하는데 비하여 총 타우는 알츠하이머병 외에도 외상성 뇌손상, 크로이트츠펠트-야콥병 등 비특이적으로 다양한 질환에서 증가 소견을 보이므로 각각 병적 타우(T), 신경퇴행(N)으로 분리하였다[31,32]. 뇌척수액 총 타우와 마찬가지로 뇌 MRI, FDG-PET와 같은 신경퇴행의 생물표지자는 알츠하이머병 외의 다른 원인에 의해서도 이상을 보일 수 있으므로, 알츠하이머병 특이 지표 그룹인 아밀로이드병증(A)이나 병적 타우(T)와 구분하여 괄호를 사용하여 표기하였다[AT(N)] [33-36].
현재의 NIA-AA Research Framework에서는 AT(N) 체계를 기점으로 TAR DNA binding protein 43, 알파-시누클레인(alphasynuclein), 은친화과립(argyrophilic grain), 해마경화증(hippocampal sclerosis), 혈관병증 등과 같이 고유의 병리 소견을 갖는 지표들도 추후 타당성이 검증되면 새로운 생물표지자 범주로 추가 확장할 예정이다. 이러한 새로운 생물표지자에 의한 확장 가능성을 ‘X’로 표현하여, AT(N)을 개념적으로는 ‘ATX(N) 체계’로 받아들일 것을 제안하고 있다. 결국 앞으로의 연구는 여러 생물표지자로 표현되는 다양한 신경병리의 상호작용을 이해하는 방향으로 나아가야 할 것이다[37].
5. 인지 단계
인지기능도 생물표지자처럼 연속적인 스펙트럼(cognitive continuum)으로 인식하고 접근하고자 하였고, 관찰 연구(observational study)와 임상 연구(clinical trial), 두 가지 상황으로 나누어서 제안하였다.
1) 관찰 연구를 위한 증상 기반 범주형 인지 단계
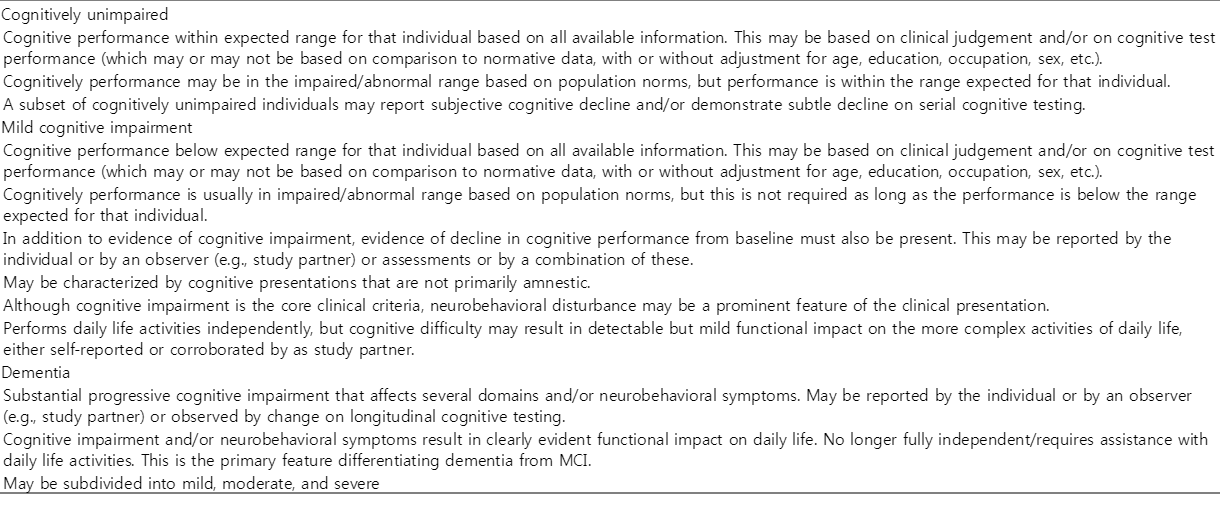
관찰 연구는 알츠하이머병 외에도 정상 생물표지자 및 알츠하이머가 아닌 다른 병리 소견을 갖는 대상자(SNAP)가 포함되므로 전통적으로 사용하던 인지장애가 없는 군(cognitively unimpaired), 경도 인지장애(mild cognitive impairment, MCI), 치매(dementia)의 세 단계로 나누는 ‘증상에 기반한 범주형 인지장애 단계’를 제안하였다(Table 3). 각 연구 대상자들에게 이러한 범주형 인지 단계와 앞서 언급한 생물표지자에 의한 분류를 서로 독립적으로 적용하여, ‘같은 인지 단계-서로 다른 생물표지자’를 갖는 경우와 ‘같은 생물표지자-서로 다른 인지 단계’를 갖는 모든 조합을 포함하고 있다(Table 4). 또한, 2011년의 NIA-AA 진단기준에서 사용하던 ‘알츠하이머병에 의한 경도인지장애(MCI due to AD)’ [4]라는 용어도 ‘경도인지장애 단계의 알츠하이머병(AD with MCI)’이라고 수정하였으며, 이는 알츠하이머병을 우선 생물표지자로 정의하고 그 다음에 대상자의 인지 단계를 추가하여, 경도인지장애의 원인을 AD만으로 한정하지 않기 위한 의도가 담겨 있다. 경도인지장애 단계의 알츠하이머병의 명명법과 관련해서는 International Working Group에서 사용한 ‘알츠하이머병 전단계(prodromal AD)’ [38]라는 용어도 병기하였고, 아예 기술하는 문구를 사용하지 않고 생물표지자와 인지 단계의 조합을 통하여 ‘A+T+(N)+ 경도인지장애’와 같이 명명하는 방법도 하나의 대안으로 제안하였다.

2) 임상 연구를 위한 숫자형 임상 단계
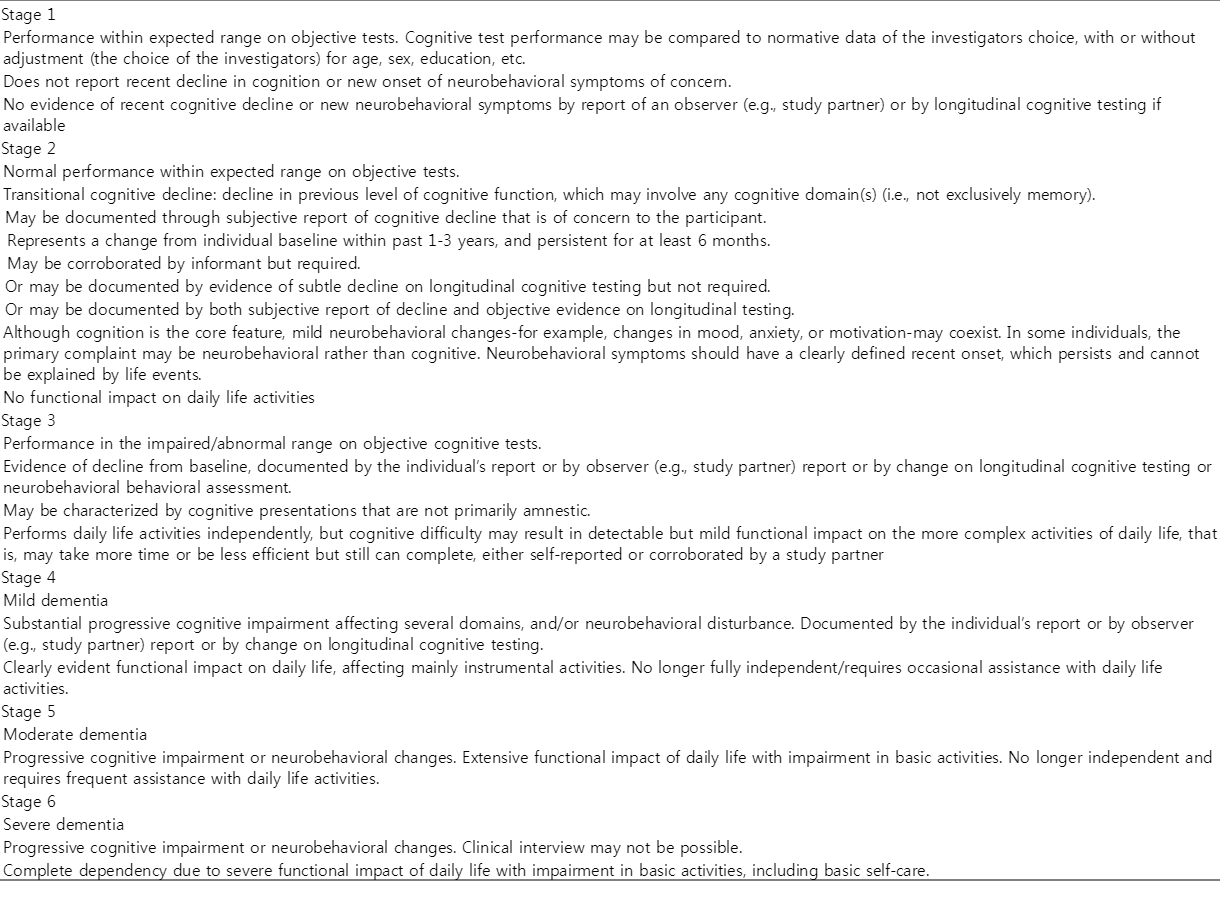
임상 연구의 경우에는 생물표지자를 바탕으로 선별된 Alzheimer’s continuum [A+T-(N)-, A+T+(N)-, A+T-(N)+, A+T+(N)+]을 대상으로 중재적 임상 실험을 시행하게 되는 경우를 상정하여 6단계로 세분화한 임상 단계(numeric clinical staging)를 제안하였다(Table 5). 총 6단계 중 임상증상이 없는 1단계, 최초로 임상증상이 탐지되는 2단계, 인지기능 저하는 있으나 기능의 소실은 없는 3단계와 다영역 인지장애와 진행하는 기능저하를 포함하는 4-6단계로 나누었다. 인지 기능의 장애는 기억력 이외의 인지기능 장애도 포함하였으며 신경행동증상만 있는 경우도 2단계에는 포함될 수 있고 3단계 이상에서는 인지기능 저하를 동반해야 한다. 모든 단계에 걸쳐 인지기능의 저하를 규준 집단과의 비교를 통하여 평가할 수 있으며 나이, 성별, 교육 등을 보정할지는 연구자의 선택에 맡겼다.
6. 기타
본 Research Framework에서는 생물표지자의 세부적인 내용을 규정하지는 않았다. 예를 들어, PET과 MRI의 이상 여부를 시각척도나 정량 분석 중 어떤 방법으로 할지, 차단점을 정할 때 나이를 고려할지 등 개별 생물표지자의 구체적인 내용에 대해서는 각각 진행 중인 연구 그룹에서 적합한 표준을 제시해 줄 것을 기대하고 있다. 또한, 생물표지자로 검출할 수 있는 신경병리 소견에 초점을 맞추고 있기 때문에 유전자는 포함시키고 있지 않다. 그리고 Research Framework가 알츠하이머병의 생물학적 정의에 초점을 맞추고 있지만, 대규모 인구 집단 및 지역사회 기반 코호트 연구 등과 같이 임상증상에 기반한 위험인자를 찾으려는 연구에 있어서까지 고비용의 PET나 침습적인 뇌척수액 생물표지자가 반드시 필요한 것은 아니라는 점도 언급하고 있다. 앞으로 개발될 것으로 기대하고 있는 저비용, 비침습적인 생물표지자가 현재로서는 생물표지자 사용이 어려운 대상 집단에게도 적용 범위를 확대시키고 임상 영역에서의 활용도를 높일 것으로 예상하고 있다[39-41]. 현재까지의 근거 우위에 따라 ‘수정된 아밀로이드 가설(modified amyloid cascade hypothesis)’에 기반하여 만든 연구를 위한 틀이지만, 생물표지자에 기반한 분류 체계를 이용하기만 한다면 인지기능 저하를 야기하는 다른 형태의 가설 검정에도 사용할 수 있는 유연성 있는 열린 연구의 틀이라는 점을 강조하고 있다.
결 론
2018년 NIA-AA Research Framework는 알츠하이머병을 생물학적으로 정의하고 있고 인지기능의 손상은 이러한 질병에 의하여 야기된 증상/징후로서 분리하여 다룬다. 연구 그룹들이 알츠하이머병을 동일한 기준으로 정의하고 의사소통을 할 수 있도록 용어를 통일하려는 노력을 하였으며, 이를 통하여 알츠하이머병의 이해를 증진시키고 치매의 다양한 원인에 대한 생물학적인 접근을 촉진할 것이라고 기대한다. 아직까지는 오직 연구를 위한 분류라는 점을 강조하고 있으나, 알츠하이머병을 정의하는데 사용되는 생물표지자들의 지속적인 타당성 검증 및 기존의 단점을 보완한 새로운 생물표지자들의 개발을 통하여 임상 분야에서의 적용이 가능해질 것으로 기대한다.