허혈뇌졸중 환자에서 두개내외동맥협착 동반에 대한 4가지 발목상완지수계산법의 비교
Comparison of Four Methods calculating Ankle Brachial Indexes for Coexistent Intracranial and Extracranial Artery Stenoses in the Patients with Ischemic Stroke
Article information
Trans Abstract
Background
The ankle brachial index (ABI) is a useful screening tool for peripheral arterial disease. It has been documented that the cerebral atherosclerosis is more frequent in stroke patients with abnormal ABI than in those with normal ABI. The present study compared the different calculation methods of ABI for coexistent intracranial and extracranial arterial stenosis (IECAS) in ischemic stroke.
Methods
We reviewed the data of patients admitted for acute ischemic stroke or transient ischemic attack. The following four distinct ABIs were calculated: the ratio of the higher (ABI-H), lower (ABI-L), or either of the systolic blood pressures (SBPs) of the posterior tibial (ABI-PT) and dorsalis pedis (ABI-DP) arteries relative to the higher of the brachial SBP. We compared the values of these four ABI measures relative to the presence of any IECAS using receiver operating characteristic (ROC) curve analysis.
Results
ABI-H, ABI-L, ABI-PT, and ABI-DP were abnormal (≤ 0.9) in 19 (13.1%), 36 (24.8%), 29 (20%), and 30 (20.7%) of 145 patients, respectively. The area under the ROC curve was significantly larger for ABI-H, ABI-L, and ABI-DP than for ABI-PT for any type of IECAS. The extracranial stenosis was more frequent when any of the four ABIs was abnormal, while intracranial stenosis was not correlated with the four ABIs. The IECAS was more frequent for abnormal ABI-H and ABI-DP than for normal ABIs.
Conclusions
Our studies suggested that ABIs based on a higher SBP of the PT or DP (i.e., ABI-H) are more strongly associated with the presence of IECAS than are those using the SBP of the PT (ABI-PT). Extracranial artery stenosis seems to be more strongly associated with ABI than is intracranial stenosis.
서 론
말초동맥질환은 팔다리 특히 다리동맥의 협착 또는 폐색으로 인해 통증, 절뚝거림, 괴사 증상을 일으키는 질환이다. 말초동맥질환은 죽상경화에 의한 동맥협착이라는 점에서 허혈뇌졸중과 공통된 병리기전을 가지고 있고, 실제로 과거 대규모연구에서 뇌졸중과 말초동맥질환은 유병률을 상당부분 공유하고 있다고 알려져 있다[1]. 말초동맥질환은 발목상완지수(ankle brachial index, ABI)를 측정함으로써 무증상말초동맥 질환까지 쉽게 선별할 수 있다[2]. 최근에는 뇌졸중 환자의 ABI에 대한 연구가 많이 이루어졌는데 뇌졸중 환자의 7-30%에서 비정상 ABI를 보였고, 비정상 ABI를 가진 뇌졸중 환자가 정상 ABI를 가진 뇌졸중 환자보다 뇌혈관협착, 뇌졸중 재발, 사망률이 더 높고 기능 회복은 더 나쁜 것으로 보고되었다[3-13].
말초동맥질환 진료지침에 따른 ABI 계산법은 한쪽 뒤정강(posterior tibial, PT)동맥과 발등(dorsalis pedis, DP)동맥에서 측정한 수축기혈압 중 높은 수치를 양쪽 위팔(brachial)동맥에서 측정한 수축기혈압 중 높은 수치로 나누는 방법이다[14,15]. PT와 DP 수축기혈압 중 낮은 수치가 아니라 높은 수치를 사용하는 이유는 PT와 DP 동맥 중 하나만 유지되어도 말초동맥질환 증상이 발생하지 않을 것이기 때문으로 알려져 있다. 한편 몇몇 연구에서는 말초동맥질환이 의심되는 환자에서 PT와 DP 혈압 중 낮은 수치를 사용하는 ABI 계산법이 높은 수치를 사용하는 ABI 계산법보다 말초동맥협착을 예측하는데 더 민감하다고 보고하였다[16]. 또 다른 한 연구에서 뇌혈관협착 동반을 예측하는데 ABI 측정이 도움이 되는 것으로 보고되었지만[3] 어떤 ABI 계산법이 더 좋은지는 알려져 있지않다. 이에 본 연구는 허혈뇌졸중 환자에서 두개내외동맥협착 동반에 대해 ABI 계산법들을 서로 비교하고자 하였다.
대상과 방법
1. 대상
2011년 4월부터 2012년 1월까지 대구가톨릭대학교병원에 급성뇌경색 또는 일과성허혈발작으로 증상 발생 일주일 이내에 입원한 환자의 임상 및 영상자료를 후향적으로 분석하였다. 급성뇌경색은 뇌확산강조영상에서 뚜렷한 급성뇌경색 소견이 관찰된 경우로 정의하였고, 일과성허혈발작은 뇌컴퓨터단층영상에서 뇌출혈이 배제된 후 뇌졸중 증상이 발생 24시간 이내에 모두 호전된 경우로 정의하였다. 연구 포함기준은 1) 20세 이상, 2) 뇌경색 또는 일과성허혈발작 증상 발생 일주일 이내에 입원한 환자였다. 연구 제외기준은 1) ABI를 측정하지 못 한 환자, 2) ABI가 1.4 초과인 환자, 3) 두개내동맥과 두개외동맥의 영상검사를 모두 실시하지 못한 환자였다. 본 연구는 본 기관의 임상연구위원회의 심사를 통과하였고 과거 진료기록지와 영상정보를 이용한 연구여서 서면동의서는 면제를 승인 받은 연구였다.
2. 방법
ABI는 환자 입원기간 중에 측정되었는데 환자 임상정보에 눈가림된 한 명의 검사자가 총 여섯 곳(양쪽 PT, DP, 위팔동맥)을 혈압띠로 감았다가 풀면서 초음파(Diagnostic Ultrasound System iU22, Philips Medical System, Bothell, WA, USA)로 감시하면서 혈압계를 보고 수축기혈압을 측정하였다. 이렇게 측정한 여섯 곳의 수치를 사용하여 4가지 다른 계산법으로 ABI를 구하였는데, 양쪽 위팔동맥 혈압 중 높은 수치를 분모로 하여 PT와 DP 혈압 중 높은 수치를 나누는 방법(ankle brachial index-higher, ABI-H), PT와 DP 혈압 중 낮은 수치를 나누는 방법(ankle brachial index-lower, ABI-L), PT 혈압 수치를 나누는 방법(ankle brachial index-posterior tibialis, ABI-PT), DP 혈압 수치를 나누는 방법(ankle brachial index-dorsalis pedis, ABI-DP)으로 계산하였다. 실제로 일부 의료기관에서 사용중인 ABI 자동측정기계는 ABI-PT 방법을 사용하고 있어 ABI-PT와 ABI-DP를 포함하여 4가지 ABI로 분석하게 되었다. 한 환자에서 측정된 양쪽 ABI 중 낮은 ABI를 지표로 삼아 비정상 ABI 유무를 정하였다. ABI가 0.9 이하인 경우를 비정상으로 정의하였고 1.4를 초과한 경우는 연구에서 제외하였다.
두개내외동맥협착은 자기공명혈관검사(magnetic resonance angiography, MRA) 또는 컴퓨터단층혈관조영술(computed tomography angiography, CTA) 영상을 이용하여 협착의 위치와 개수를 측정하였다. 두개내외동맥협착 외에 좀 더 세분하여 두개외동맥, 두개내동맥, 목동맥, 척추동맥, 앞순환동맥, 뒤순환동맥, 다발동맥협착으로 분류하였다. 두개외동맥은 속목동맥, 온목동맥, 척추동맥의 두개외 부분으로 정의하였고 50% 이상 협착을 의미 있는 협착으로 판단하였다. 영상분석은 두 명의 신경과 의사가 환자 임상정보에 눈가림된 상태로 독립적으로 시행하였다. 두 명의 판단이 다른 경우에는 제 3의 신경과 의사에게 의뢰한 후 서로 합의하여 결정하였다.
그 외에 변수가 되는 환자의 임상정보로 나이, 성별, 고혈압, 당뇨병, 고지혈증, 관상동맥질환, 심장성색전 원인질환 유무, 흡연, 입원 시 NIH 뇌졸중척도(National Institute of Health Stroke Scale, NIHSS), 뇌졸중 아형을 조사하였다.
3. 분석방법
말초동맥질환 진료지침 계산법인 ABI-H가 비정상인 환자군과 정상인 환자군의 임상정보를 비교하였는데 범주형변수는 카이제곱검정 또는 Fisher 정확검증을, 연속형변수는 스투덴트t검정을 사용하였다. 4가지 ABI 각각의 비정상군과 정상군의 두개내외동맥 협착을 카이제곱검정 또는 Fisher 정확검증을 사용하여 비교하였다. 심장성색전 원인질환을 가진 환자에서는 혈관협착이 죽상경화성 변화인지 색전증에 의한 것인지 구별하기 어려우므로 심장성색전 원인질환을 가진 환자를 제외한 환자들을 대상으로도 4가지 ABI 정상군과 비정상군 간의 동맥협착을 비교하였다. 두개내동맥협착 여부와 두개외동맥협착 여부에 따라 4가지 ABI와 환자의 임상정보를 비교하였다. 4가지 ABI를 서로 비교하기 위해서 수신기 작동특성곡선(receiver-operating characteristic curve, ROC)분석과 ROC 곡선 짝비교(pairwise comparison)를 사용하여 두개내외동맥협착과 두개외동맥협착에 대하여 4가지 ABI를 비교하였다. 통계분석은 SPSS for Windows, Version 18.0 (SPSS Inc., Chicago, IL, USA)와 MedCalc software, Version 12.3 (MedCalc Inc., Mariakerke, Belgium)을 사용하였고, 통계적 유의수준은 p<0.05로 정하였다.
결 과
2011년 4월부터 2012년 1월까지 386명이 연구 포함기준에 해당하는 뇌경색 또는 일과성허혈발작으로 입원하였다. 386명 중 뇌졸중 증상이 심하거나 입원기간 중에 실시하지 못한 환자 157명, ABI가 1.4 초과인 환자 0명, 두개내외혈관영상이 모두 시행되지 않은 환자 84명이 제외되어 최종적으로 145명을 분석하였다. 비정상 ABI-H를 가진 환자는 정상 ABI-H 환자보다 나이가 더 많고 당뇨병과 관상동맥질환을 더 많이 가지고 있었고 입원 시 NIHSS 점수가 더 높았다(Table 1). 비정상 ABI-H, ABI-L, ABI-PT, ABI-DP 환자는 각각 19 (13.1%), 36 (24.8%), 29 (20%), 30 (20.7%)명이었다. 두개내외동맥협착은 ABI-H와 ABI-DP를 사용했을 때 비정상 환자에서 정상 환자보다 더 많았던 반면 ABI-L와 ABI-PT를 사용했을 때는 비정상 환자와 정상 환자 사이에 두개내외동맥협착의 차이가 없었다. 두개내동맥협착은 4가지 ABI 모두에서 비정상 환자와 정상 환자 사이에 차이가 없었고, 두개외동맥협착은 4가지 ABI 모두에서 비정상 환자가 정상 환자보다 더 많았다. 이러한 결과는 심장성색전 원인질환을 가진 환자 13명을 제외한 환자들을 대상으로 분석하여도 비슷한 결과였다(Table 2). 두개내동맥협착을 가진 환자군은 두개내동맥협착이 없는 환자군에 비해 여성이 더 많았고 고혈압이 더 많았으나 4가지 ABI는 차이가 없었다. 반면 두개외동맥협착을 가진 환자군은 두개외동맥협착이 없는 환자군에 비해 나이가 더 많았고 관상동맥질환이 더 많았으며 4가지 ABI 모두에서 비정상인 환자가 유의하게 더 많았다(Table 3). ROC 곡선 짝비교 결과, 두개내외동맥협착은 ABI-H, ABI-L, ABI-DP가 ABI-PT보다 유의하게 area under curve (AUC)가 더 높았다. 두개외동맥협착도 ABI-H, ABI-L, ABI-DP가 ABI-PT보다 유의하게 더 높은 AUC를 보였다(Fig.).
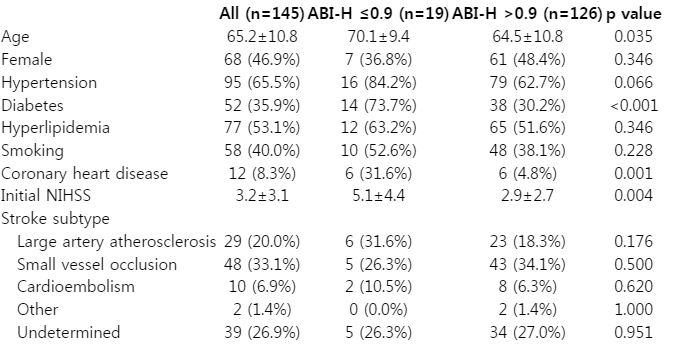
Characteristics of the patients
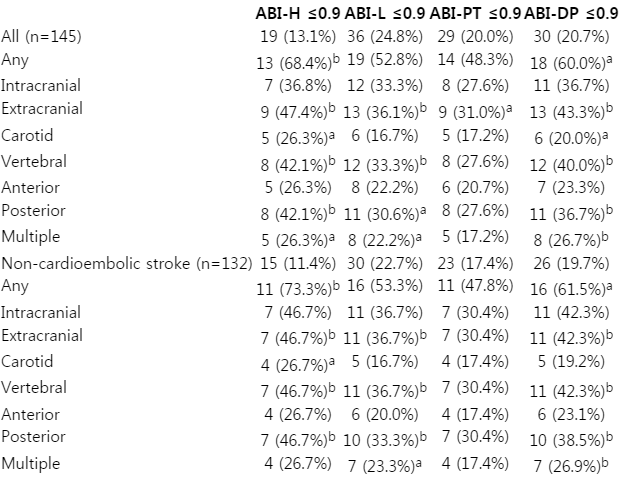
Coexistent intracranial and extracranial artery stenosis in each four ankle-brachial indexes
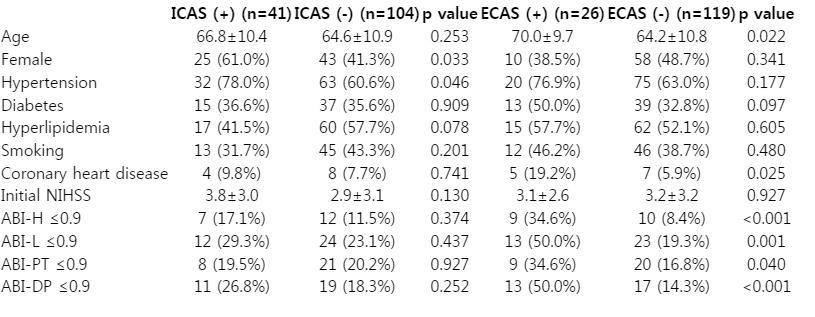
Four ankle-brachial indexes and characteristics of the patients according to the presence of intracranial or extracranial artery stenosis

Comparison of four different ankle brachial indexes for coexistent intracranial and extracranial artery stenosis. Receiver-operator characteristic curve analysis with pairwise comparison showed that ABI-H, ABI-L, and ABI-DP had significantly higher area under curve than ABI-PT for the presence of any intracranial and extracranial artery stenosis (A) and extracranial artery stenosis (B). ABI-H; ankle brachial index-higher, ABI-L; ankle brachial index-lower, ABI-PT; ankle brachial index-posterior tibialis, ABI-DP; ankle brachial index-dorsalis pedis, AUC; area under curve.
고 찰
본 연구는 뇌졸중 환자에서 진료지침에 따른 ABI 계산법(ABI-H)은 다른 ABI 계산법에 비해 두개내외동맥협착 동반에 대해 차이가 없었고, 다른 ABI 계산법 중 PT 수축기혈압을 이용한 ABI 계산법(ABI-PT)에 비해서는 더 민감하다는 결과를 보여주었다. ABI는 주로 무증상말초동맥질환을 선별하는 용도로 많이 사용하는데 PT 또는 DP 중 높은 수치를 사용하는 이유는 PT와 DP 동맥 중 하나만 유지되어도 말초동맥질환 증상이 발생하지 않을 것이기 때문인 반면, PT 또는 DP 동맥 중 낮은 혈압을 이용하면 높은 혈압을 이용하는 방법보다 말초동맥질환뿐만 아니라 다른 동맥경화질환을 예측하는데 민감도가 더 좋을 것으로 생각되어져 왔다. 이에 관한 이전 연구에서는 일차진료환자에서 ABI-H가 다른 ABI계산법보다 말초동맥질환을 예측하는데 우월하였고 심혈관사건을 예측하는데 동등하다고 보고하였다[17]. 반면 말초동맥질환이 의심되는 환자와[16] 관상동맥질환 환자를[18] 대상으로 한 연구에서는 ABI-L이 ABI-H보다 말초동맥질환을 예측하고 심혈관사건 발생을 예측하는데 더 좋은 것으로 보고하여 환자 대상과 측정 결과에 따라 ABI 계산법 우열이 달랐다. 뇌경색 환자를 대상으로 ABI 계산법을 비교한 연구는 없었는데 본 연구에서는 두개내외동맥협착 동반에 대해 ABI-H가 다른 ABI 계산법보다 더 선호될 수 있겠다. 하지만 ABI-H가 ABI-PT에 비해 더 좋은 이유는 알 수 없었다.
비정상 ABI-H가 두개내동맥협착과는 관계가 없고 두개외동맥협착과 관계가 있음을 본 연구에서 보였다. 두개외죽상경화와 두개내죽상경화의 기전에는 차이가 있는 것으로 알려져 있는데, 두개외혈관은 대동맥이나 빗장밑동맥, 엉덩동맥 등 전신혈관과 혈관벽의 구조가 유사한 반면 두개내혈관은 바깥탄력막이 없고 중막층에는 탄력섬유조직이 적으며 바깥막이 얇아서 탄력성이 두개외혈관에 비해 적은 차이점이 있다. 실제로 두개외협착 환자에서 관상동맥질환이 자주 동반되는 반면 두개내동맥협착이 있는 경우는 두개외동맥협착보다는 다른 두개내혈관협착을 흔히 동반하는 것으로 알려져 있다[19]. 말초동맥질환도 관상동맥질환과 마찬가지로 두개외동맥협착과 연관이 있을 것으로 생각할 수 있는데 본 연구결과도 두개외혈관협착만 말초동맥질환과 관계 있었다. 이전 연구들에서는 비정상 ABI가 두개외동맥협착과 일관된 연관성을 보였으나 두개내동맥협착과는 일관된 연관성이 없었는데, 일부 연구에서는 협착 정도에 관계 없이 모든 정도의 두개내동맥협착은 비정상 ABI와 무관하였고[5,6], 다른 일부 연구에서는 50% 이상의 두개내동맥협착은 비정상 ABI와 연관성이 있었다[7]. 하지만 이 연구들은 대부분 초음파만으로 동맥협착을 측정하여 두개내동맥협착을 측정하는데 제한이 있었음에 비해 본 연구는 MRA와 CTA로 두개내동맥협착을 측정하여 이전 연구에 비해 협착 측정이 더 정확할 것으로 생각된다. 무증상목동맥협착을 선별하기 위해 일률적인 목동맥혈관초음파는 뇌졸중진료지침에서도 권고되지 않으므로 ABI로 대상을 선별하고 위험인자들을 고려하여 두개외혈관검사 시행을 결정할 수 있겠다.
동양인이 서양인보다 두개내동맥협착이 더 많은 것으로 알려져 있으므로 비정상 ABI 환자가 두개내, 두개외동맥협착 모두 더 많이 동반할 것인지, 이와는 다르게 인종차이를 넘어서 두개외동맥과 두개내동맥은 병리생태기전이 다르므로 두개외동맥만이 비정상 ABI와 연관있을 것인지 몇몇 연구가 있었다. 아시아에서 행해진 연구 중 일부에서는 비정상 ABI가 두개내외동맥협착 모두와 연관있다고 보고한 반면[20] 다른 연구에서는 두개외동맥협착만 비정상 ABI와 연관있다고 보고했는데[6,21], 본 연구는 두개외동맥협착만 연관이 있었다.
비정상 ABI-H를 가진 환자가 정상 ABI-H 환자보다 나이가 더 많고, 당뇨병과 관상동맥질환 과거력이 더 많으며, 입원 시 NIHSS가 더 높은 본 연구 결과는 다른 이전 연구 결과와 같았다. 비정상 ABI-H의 빈도도 이전 연구와 비슷하였다. 말초동맥질환이 의심되는 환자 대상으로 한 이전 연구에서 말초동맥협착을 진단하는데 ABI-H의 민감도는 0.68, 특이도는 0.99였고, ABI-L의 민감도는 0.89, 특이도는 0.93인 것에 비해[16] 뇌경색 환자를 대상으로 한 본 연구에서는 두개내외동맥협착 예측하는데 특이도는 0.80-0.93으로 좋은 반면에 민감도는 0.22-0.32 정도로 많이 낮았다.
본 연구는 후향연구로 설계되었고 대상 환자수가 적었으며 배제 기준에 해당한 환자가 많았는데 주로 심장성색전증 또는 큰혈관동맥경화성 뇌경색 환자가 뇌졸중 증상이 심하거나 불안정하여 입원 중 ABI 측정이 되지 않은 환자가 많았을 것으로 생각된다. 입원환자만을 대상으로 하였고 뇌졸중 재발과 항혈전제 복용상태를 조사하지 못한 점, 그리고 적은 환자수로 인해 치우침이나 교란요인을 보정하지 못한 점이 본 연구의 제한점으로 생각된다.
결론적으로 본 연구는 진료지침에 따른 ABI 계산법이 뇌경색 환자 중 두개내외동맥경화 동반여부를 선별할 수 있는 비침습적이고 간단한 도구임을 보여준다. 특히 뇌경색 환자를 진료하지만 뇌혈관영상검사를 쉽게 권유하기 힘든 일차진료의사에게 유용할 것으로 생각된다.